

Adherence Tradeoff to Multiple Preventive Therapies and All-Cause Mortality After Acute Myocardial Infarction
- PMID: 28935030
- PMCID: PMC5890809
- DOI: 10.1016/j.jacc.2017.07.783
Adherence Tradeoff to Multiple Preventive Therapies and All-Cause Mortality After Acute Myocardial Infarction
Abstract
Background: Angiotensin-converting enzyme (ACE) inhibitors/angiotensin II receptor blockers (ARB), beta-blockers and statins are recommended after acute myocardial infarction (AMI). Patients may adhere to some, but not all, therapies.
Objectives: The authors investigated the effect of tradeoffs in adherence to ACE inhibitors/ARBs, beta-blockers, and statins on survival among older people after AMI.
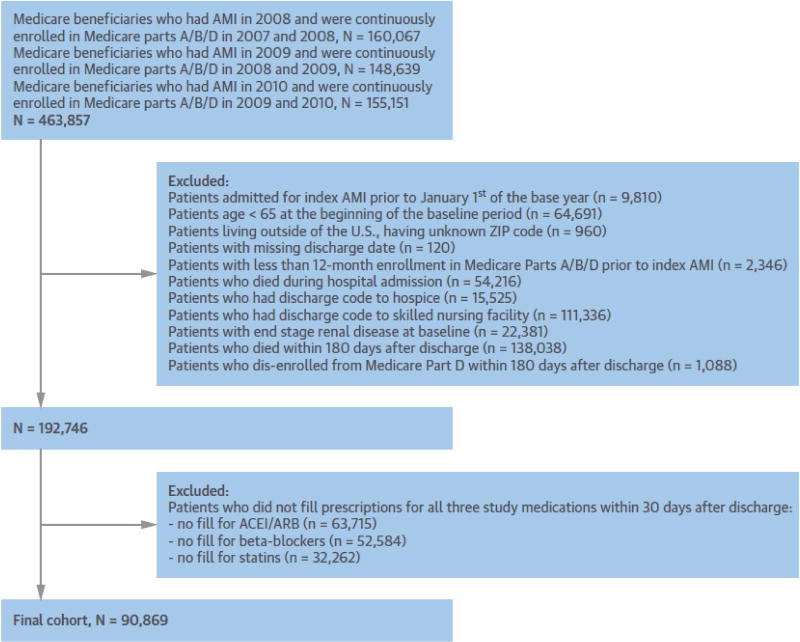
Methods: The authors identified 90,869 Medicare beneficiaries ≥65 years of age who had prescriptions for ACE inhibitors/ARBs, beta-blockers, and statins, and survived ≥180 days after AMI hospitalization in 2008 to 2010. Adherence was measured by proportion of days covered (PDC) during 180 days following hospital discharge. Mortality follow-up extended up to 18 months after this period. The authors used Cox proportional hazards models to estimate hazard ratios of mortality for groups adherent to 2, 1, or none of the therapies versus group adherent to all 3 therapies.
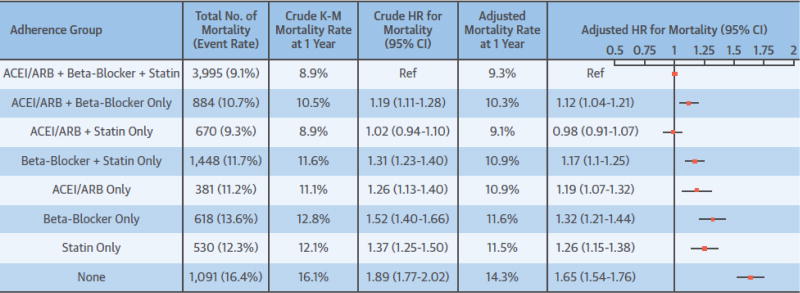
Results: Only 49% of the patients adhered (PDC ≥80%) to all 3 therapies. Compared with being adherent to all 3 therapies, multivariable-adjusted hazard ratios (95% confidence intervals [CIs]) for mortality were 1.12 (95% CI: 1.04 to 1.21) for being adherent to ACE inhibitors/ARBs and beta-blockers only, 0.98 (95% CI: 0.91 to 1.07) for ACEI/ARBs and statins only, 1.17 (95% CI: 1.10 to 1.25) beta-blockers and statins only, 1.19 (95% CI: 1.07 to 1.32) for ACE inhibitors/ARBs only, 1.32 (95% CI: 1.21 to 1.44) for beta-blockers only, 1.26 (95% CI: 1.15 to 1.38) statins only, and 1.65 (95% CI: 1.54 to 1.76) for being nonadherent (PDC <80%) to all 3 therapies.
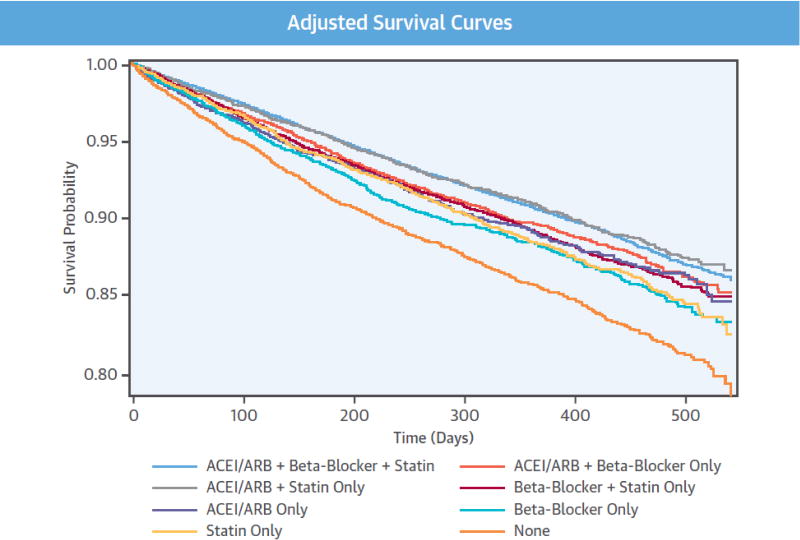
Conclusions: Patients adherent to ACE inhibitors/ARBs and statins only had similar mortality rates as those adherent to all 3 therapies, suggesting limited additional benefit for beta-blockers in patients who were adherent to statins and ACE inhibitors/ARBs. Nonadherence to ACE inhibitors/ARBs and/or statins was associated with higher mortality.
Keywords: medication adherence; myocardial infarction; older adults; secondary prevention.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
"Sticky" Issues for Adherence in Secondary Prevention.J Am Coll Cardiol. 2017 Sep 26;70(13):1555-1557. doi: 10.1016/j.jacc.2017.07.788. J Am Coll Cardiol. 2017. PMID: 28935031 No abstract available.
References
-
- Rasmussen JN, Chong A, Alter DA. Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarction. JAMA. 2007;297:177–86. - PubMed
-
- Choudhry NK, Glynn RJ, Avorn J, et al. Untangling the relationship between medication adherence and post-myocardial infarction outcomes: medication adherence and clinical outcomes. Am Heart J. 2014;167:51–8. e5. - PubMed
-
- Hamood H, Hamood R, Green MS, Almog R. Effect of adherence to evidence-based therapy after acute myocardial infarction on all-cause mortality. Pharmacoepidemiology Drug Saf. 2015;24:1093–104. - PubMed
-
- Bansilal S, Castellano JM, Garrido E, et al. Assessing the impact of medication adherence on long-term cardiovascular outcomes. J Am Coll Cardiol. 2016;68:789–801. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
