

Inferior Vena Cava Filters to Prevent Pulmonary Embolism: Systematic Review and Meta-Analysis
- PMID: 28935036
- PMCID: PMC8412839
- DOI: 10.1016/j.jacc.2017.07.775
Inferior Vena Cava Filters to Prevent Pulmonary Embolism: Systematic Review and Meta-Analysis
Abstract
Background: Inferior vena cava (IVC) filters are widely used for prevention of pulmonary embolism (PE). However, uncertainty persists about their efficacy and safety.
Objectives: The authors conducted a systematic review and meta-analysis of the published reports on the efficacy and safety of IVC filters.
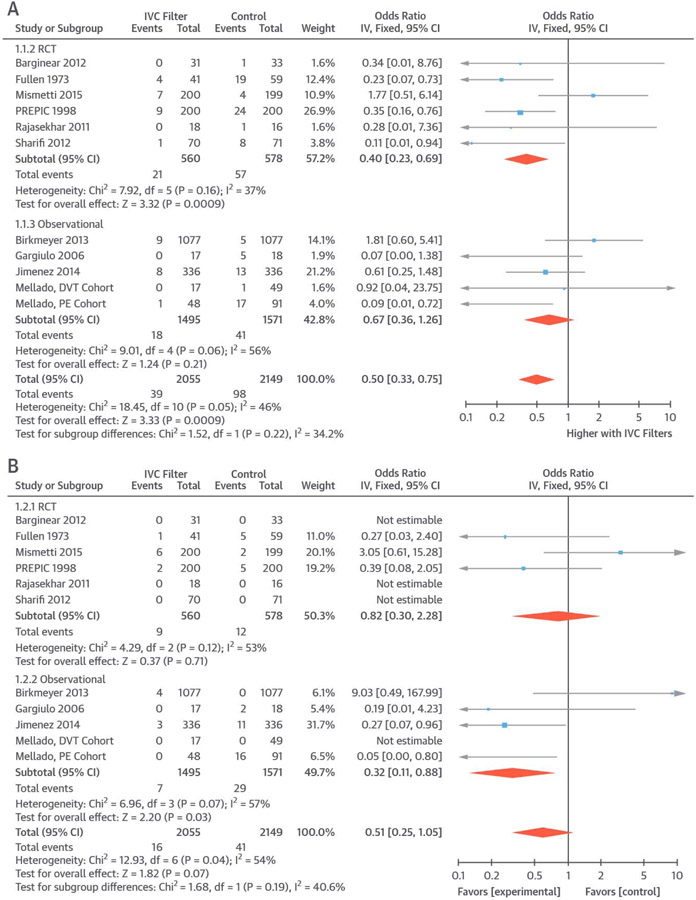
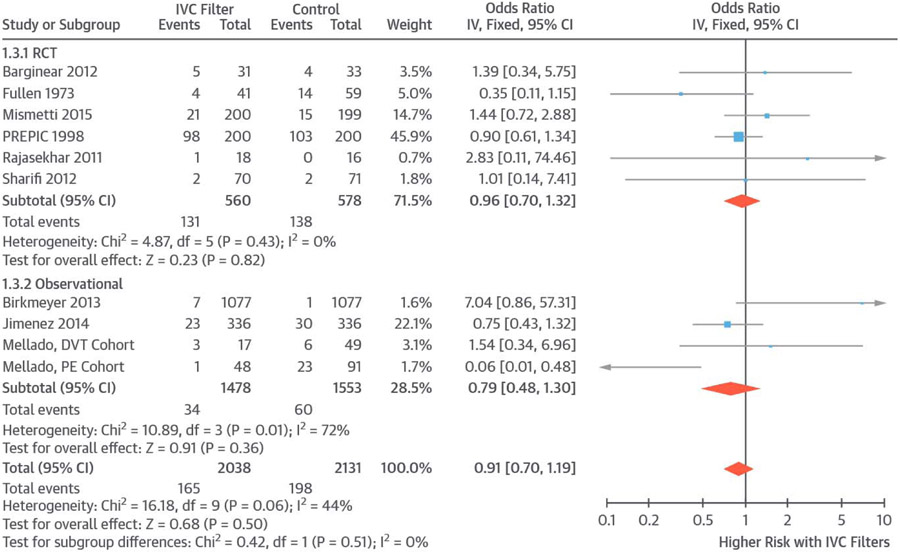
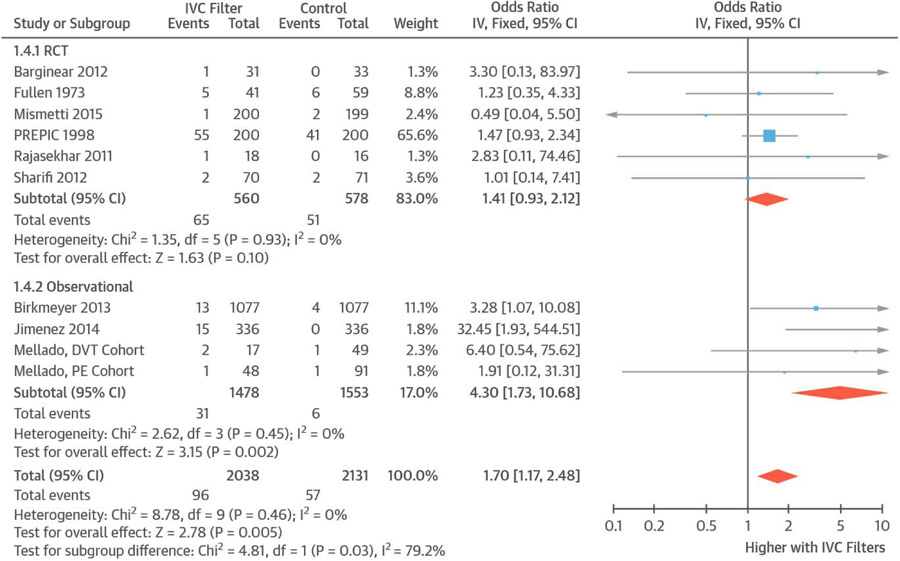
Methods: The authors searched PubMed, the Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov through October 3, 2016, for randomized controlled trials (RCTs) or prospective controlled observational studies of IVC filters versus none in patients at risk of PE. Inverse variance fixed-effects models with odds ratio (OR) as the effect measure were used for primary analyses. Main outcomes included subsequent PE, PE-related mortality, all-cause mortality, and subsequent deep vein thrombosis (DVT).
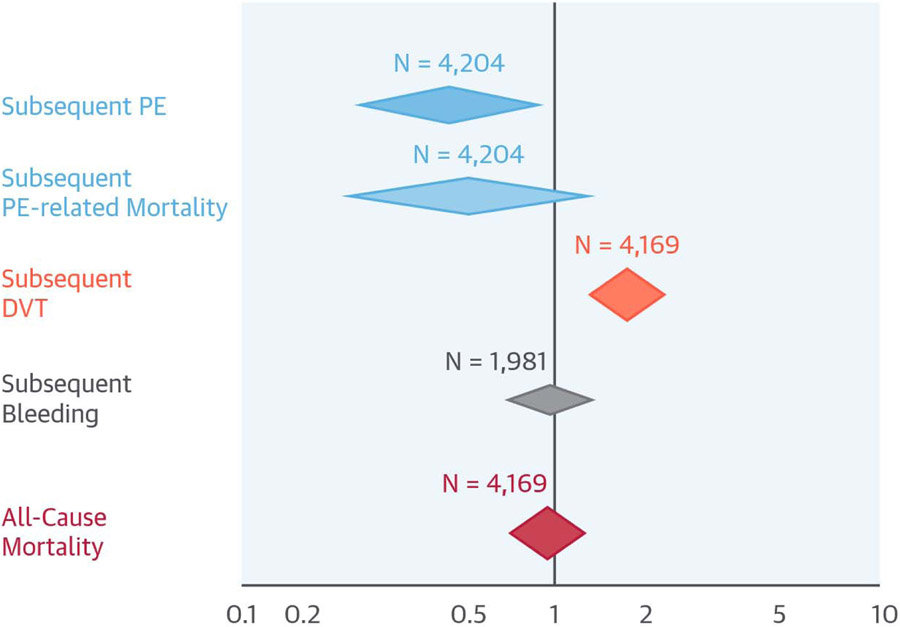
Results: The authors' search retrieved 1,986 studies, of which 11 met criteria for inclusion (6 RCTs and 5 prospective observational studies). Quality of evidence for RCTs was low to moderate. Overall, patients receiving IVC filters had lower risk for subsequent PE (OR: 0.50; 95% confidence interval [CI]: 0.33 to 0.75); increased risk for DVT (OR: 1.70; 95% CI: 1.17 to 2.48); nonsignificantly lower PE-related mortality (OR: 0.51; 95% CI: 0.25 to 1.05); and no change in all-cause mortality (OR: 0.91; 95% CI: 0.70 to 1.19). Limiting the results to RCTs showed similar results. Findings were substantively similar across a wide range of sensitivity analyses.
Conclusions: Very few prospective controlled studies, with limited quality of evidence, exist regarding the efficacy and safety of IVC filters. Overall, filters appear to reduce the risk of subsequent PE, increase the risk for DVT, and have no significant effect on overall mortality.
Keywords: bleed; mortality; prevention; risk; venous thromboembolism.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Elusive Evidence for Inferior Vena Cava Filters to Prevent Pulmonary Embolism.J Am Coll Cardiol. 2017 Sep 26;70(13):1598-1600. doi: 10.1016/j.jacc.2017.08.005. J Am Coll Cardiol. 2017. PMID: 28935037 No abstract available.
References
-
- Bikdeli B, Gupta A, Mody P, Lampropulos JF, Dharmarajan K. Most important outcomes research papers on anticoagulation for cardiovascular disease. Circ Cardiovasc Qual Outcomes 2012;5:e65–74. - PubMed
-
- Heit JA, Cohen AT, Anderson FJ. Estimated annual number of incident and recurrent, nonfatal and fatal venous thromboembolism (VTE) events in the US. Blood 2005;106:1.
-
- Cohen AT, Agnelli G, Anderson FA, et al. Venous thromboembolism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Thromb Haemost 2007;98:756–64. - PubMed
-
- Bikdeli B, Bikdeli B. Updates on advanced therapies for acute pulmonary embolism. Int J Cardiovasc Pract 2016;1:47–50.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
