

Optimising the Diagnosis of Prostate Cancer in the Era of Multiparametric Magnetic Resonance Imaging: A Cost-effectiveness Analysis Based on the Prostate MR Imaging Study (PROMIS)
- PMID: 28935163
- PMCID: PMC5718727
- DOI: 10.1016/j.eururo.2017.08.018
Optimising the Diagnosis of Prostate Cancer in the Era of Multiparametric Magnetic Resonance Imaging: A Cost-effectiveness Analysis Based on the Prostate MR Imaging Study (PROMIS)
Abstract
Background: The current recommendation of using transrectal ultrasound-guided biopsy (TRUSB) to diagnose prostate cancer misses clinically significant (CS) cancers. More sensitive biopsies (eg, template prostate mapping biopsy [TPMB]) are too resource intensive for routine use, and there is little evidence on multiparametric magnetic resonance imaging (MPMRI).
Objective: To identify the most effective and cost-effective way of using these tests to detect CS prostate cancer.
Design, setting, and participants: Cost-effectiveness modelling of health outcomes and costs of men referred to secondary care with a suspicion of prostate cancer prior to any biopsy in the UK National Health Service using information from the diagnostic Prostate MR Imaging Study (PROMIS).
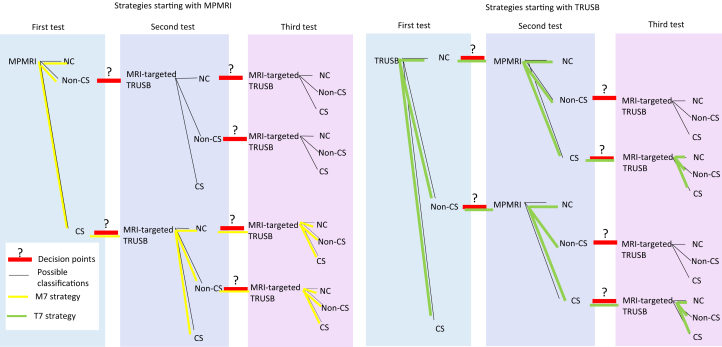
Intervention: Combinations of MPMRI, TRUSB, and TPMB, using different definitions and diagnostic cut-offs for CS cancer.
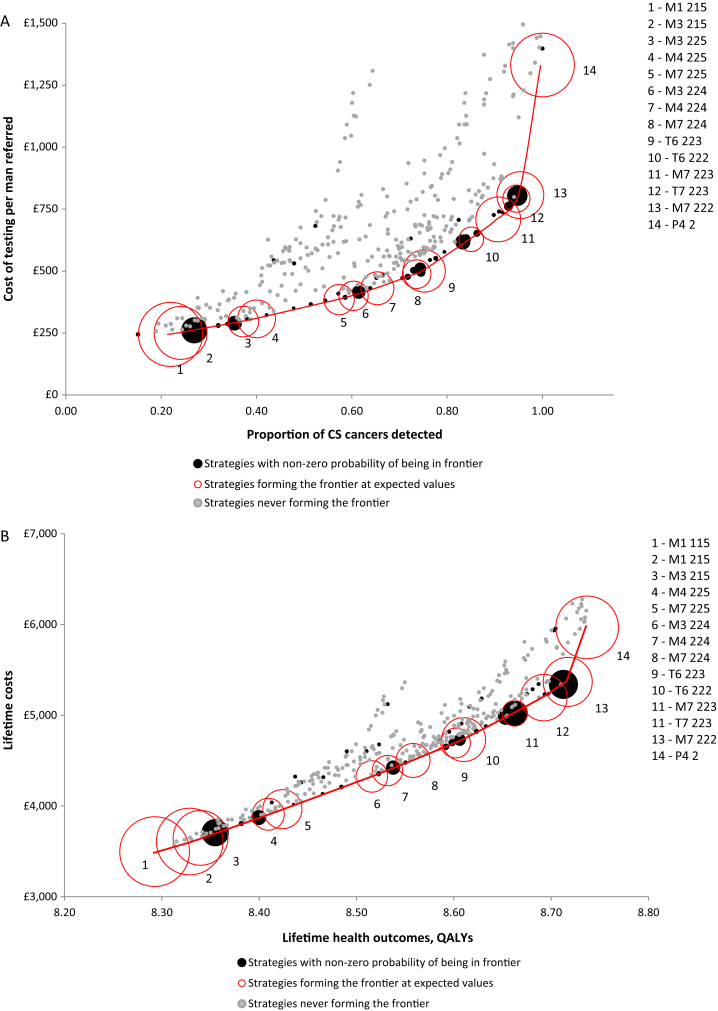
Outcome measurements and statistical analysis: Strategies that detect the most CS cancers given testing costs, and incremental cost-effectiveness ratios (ICERs) in quality-adjusted life years (QALYs) given long-term costs.
Results and limitations: The use of MPMRI first and then up to two MRI-targeted TRUSBs detects more CS cancers per pound spent than a strategy using TRUSB first (sensitivity = 0.95 [95% confidence interval {CI} 0.92-0.98] vs 0.91 [95% CI 0.86-0.94]) and is cost effective (ICER = £7,076 [€8350/QALY gained]). The limitations stem from the evidence base in the accuracy of MRI-targeted biopsy and the long-term outcomes of men with CS prostate cancer.
Conclusions: An MPMRI-first strategy is effective and cost effective for the diagnosis of CS prostate cancer. These findings are sensitive to the test costs, sensitivity of MRI-targeted TRUSB, and long-term outcomes of men with cancer, which warrant more empirical research. This analysis can inform the development of clinical guidelines.
Patient summary: We found that, under certain assumptions, the use of multiparametric magnetic resonance imaging first and then up to two transrectal ultrasound-guided biopsy is better than the current clinical standard and is good value for money.
Keywords: Cost-effectiveness analysis; Magnetic resonance imaging; Model-based analysis; Prostate biopsy; Prostate cancer.
Copyright © 2017 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
The "PROMIS" of Magnetic Resonance Imaging Cost Effectiveness in Prostate Cancer Diagnosis?Eur Urol. 2018 Jan;73(1):31-32. doi: 10.1016/j.eururo.2017.09.015. Epub 2017 Sep 29. Eur Urol. 2018. PMID: 28965689 No abstract available.
-
Imaging: MRI improves cost and accuracy of prostate cancer biopsy.Nat Rev Urol. 2018 Jan;15(1):6-8. doi: 10.1038/nrurol.2017.185. Epub 2017 Nov 8. Nat Rev Urol. 2018. PMID: 29116256 No abstract available.
-
Re: Rita Faria, Marta O. Soares, Eldon Spackman, et al. Optimising the Diagnosis of Prostate Cancer in the Era of Multiparametric Magnetic Resonance Imaging: A Cost-effectiveness Analysis Based on the Prostate MR Imaging Study (PROMIS). Eur Urol 2018;73:23-30.Eur Urol. 2018 Apr;73(4):e108-e109. doi: 10.1016/j.eururo.2017.10.035. Epub 2017 Nov 11. Eur Urol. 2018. PMID: 29132712 No abstract available.
-
Re: Jochen Walz. The "PROMIS" of Magnetic Resonance Imaging Cost Effectiveness in Prostate Cancer Diagnosis? Eur Urol 2018;73:31-2.Eur Urol. 2018 Jun;73(6):e151-e152. doi: 10.1016/j.eururo.2018.02.003. Epub 2018 Feb 17. Eur Urol. 2018. PMID: 29463435 No abstract available.
-
Re: Optimising the Diagnosis of Prostate Cancer in the Era of Multiparametric Magnetic Resonance Imaging: A Cost-Effectiveness Analysis Based on the Prostate MR Imaging Study (PROMIS).J Urol. 2018 Jun;199(6):1397-1398. doi: 10.1016/j.juro.2018.03.027. Epub 2018 Mar 16. J Urol. 2018. PMID: 29783593 No abstract available.
References
-
- National Institute for Health and Care Excellence (NICE) NICE; London, UK: 2014. Prostate cancer: diagnosis and management. Clinical guideline.
-
- Mottet N., Bellmunt J., Briers E. European Association of Urology; 2015. Guidelines on Prostate Cancer.
-
- Fütterer J.J., Briganti A., De Visschere P. Can clinically significant prostate cancer be detected with multiparametric magnetic resonance imaging? A systematic review of the literature. Eur Urol. 2015;68:1045–1053. - PubMed
-
- Thompson J., van Leeuwen P., Moses D. The diagnostic performance of multiparametric magnetic resonance imaging to detect significant prostate cancer. J Urol. 2016;195:1428–1435. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
