

Particulate Matter Air Pollution and the Risk of Incident CKD and Progression to ESRD
- PMID: 28935655
- PMCID: PMC5748906
- DOI: 10.1681/ASN.2017030253
Particulate Matter Air Pollution and the Risk of Incident CKD and Progression to ESRD
Abstract
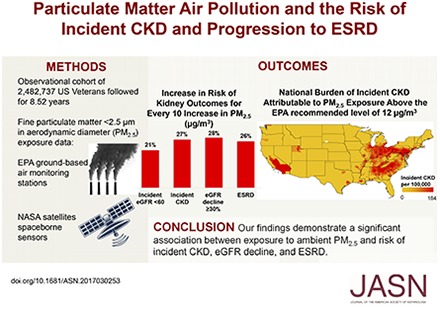
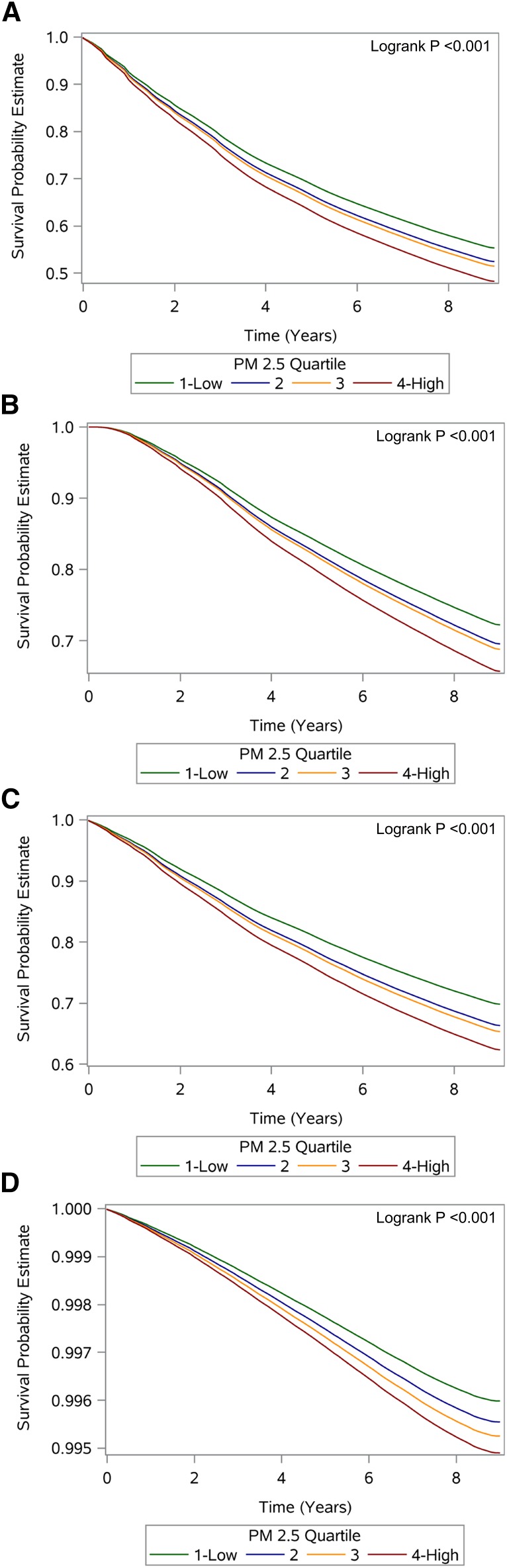
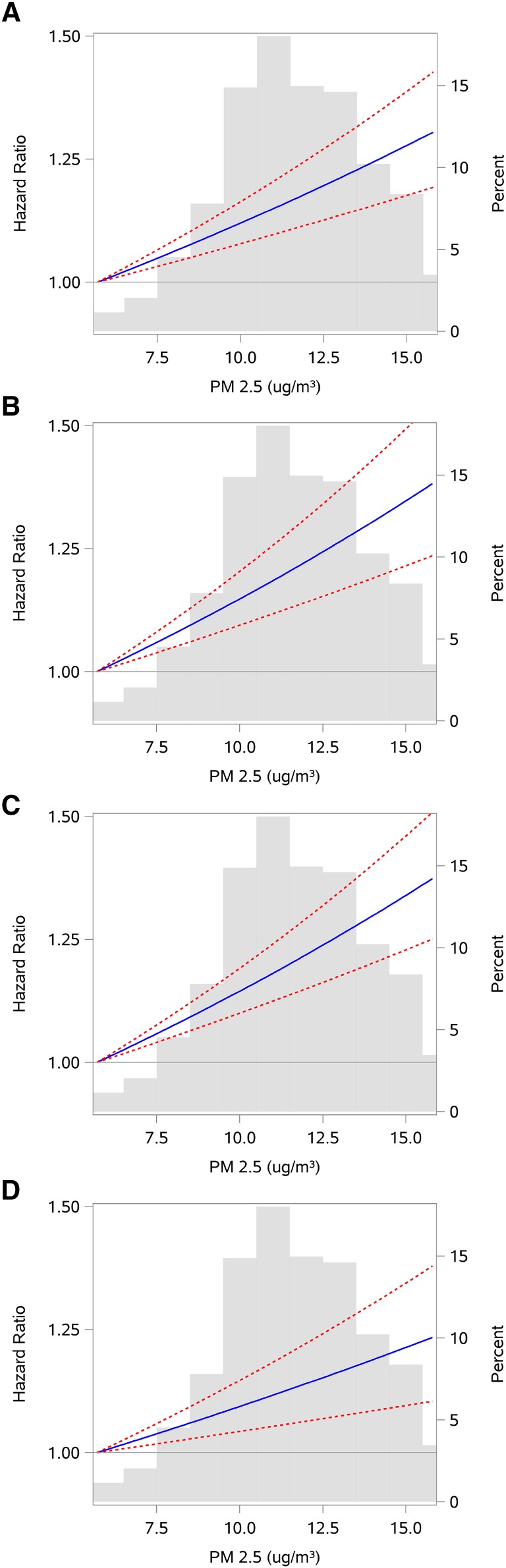
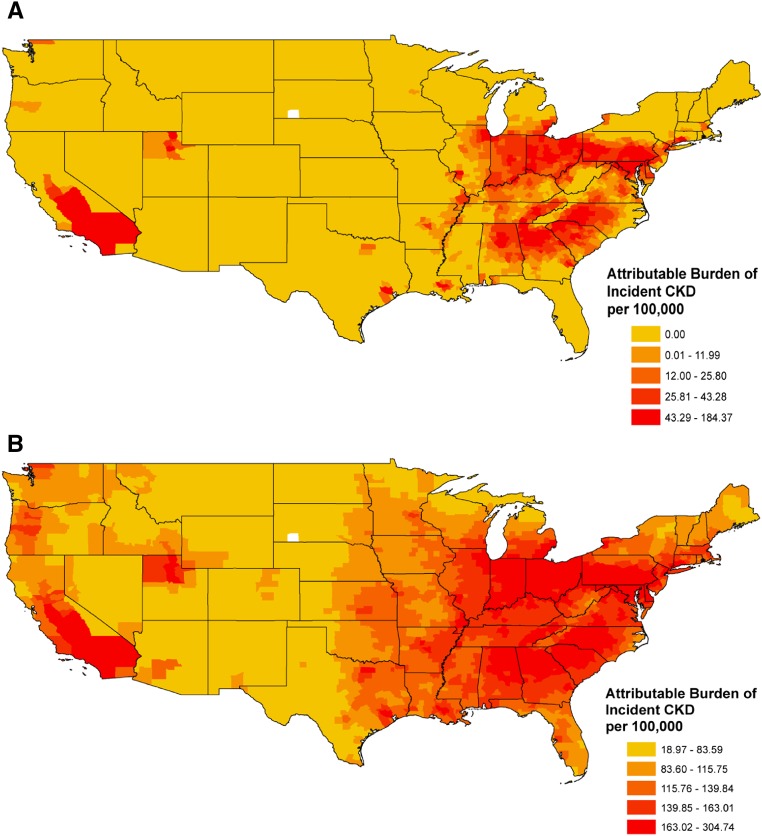
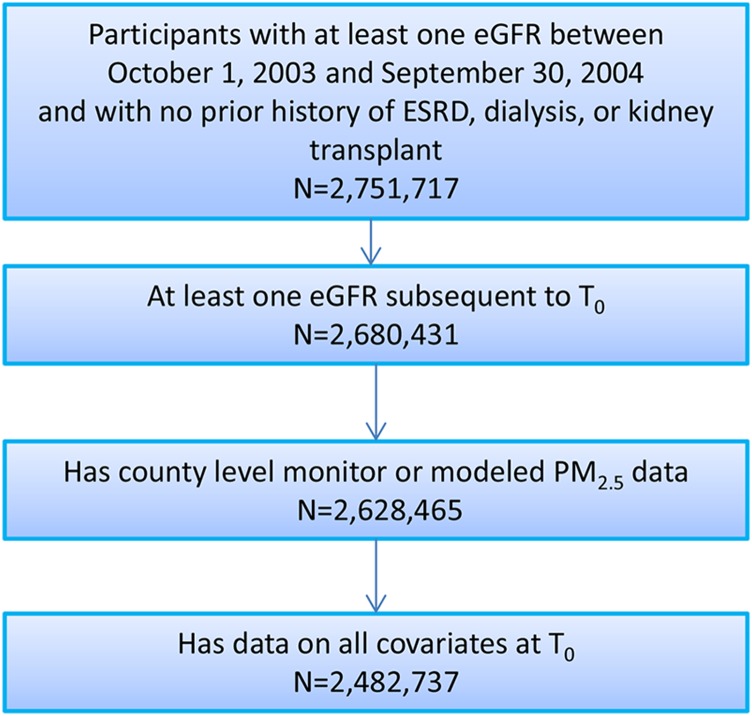
Elevated levels of fine particulate matter <2.5 µm in aerodynamic diameter (PM2.5) are associated with increased risk of cardiovascular outcomes and death, but their association with risk of CKD and ESRD is unknown. We linked the Environmental Protection Agency and the Department of Veterans Affairs databases to build an observational cohort of 2,482,737 United States veterans, and used survival models to evaluate the association of PM2.5 concentrations and risk of incident eGFR <60 ml/min per 1.73 m2, incident CKD, eGFR decline ≥30%, and ESRD over a median follow-up of 8.52 years. County-level exposure was defined at baseline as the annual average PM2.5 concentrations in 2004, and separately as time-varying where it was updated annually and as cohort participants moved. In analyses of baseline exposure (median, 11.8 [interquartile range, 10.1-13.7] µg/m3), a 10-µg/m3 increase in PM2.5 concentration was associated with increased risk of eGFR<60 ml/min per 1.73 m2 (hazard ratio [HR], 1.21; 95% confidence interval [95% CI], 1.14 to 1.29), CKD (HR, 1.27; 95% CI, 1.17 to 1.38), eGFR decline ≥30% (HR, 1.28; 95% CI, 1.18 to 1.39), and ESRD (HR, 1.26; 95% CI, 1.17 to 1.35). In time-varying analyses, a 10-µg/m3 increase in PM2.5 concentration was associated with similarly increased risk of eGFR<60 ml/min per 1.73 m2, CKD, eGFR decline ≥30%, and ESRD. Spline analyses showed a linear relationship between PM2.5 concentrations and risk of kidney outcomes. Exposure estimates derived from National Aeronautics and Space Administration satellite data yielded consistent results. Our findings demonstrate a significant association between exposure to PM2.5 and risk of incident CKD, eGFR decline, and ESRD.
Keywords: ESRD; chronic kidney disease; glomerular filtration rate.
Copyright © 2018 by the American Society of Nephrology.
Figures
References
-
- Mateen FJ, Brook RD: Air pollution as an emerging global risk factor for stroke. JAMA 305: 1240–1241, 2011 - PubMed
-
- Miller KA, Siscovick DS, Sheppard L, Shepherd K, Sullivan JH, Anderson GL, Kaufman JD: Long-term exposure to air pollution and incidence of cardiovascular events in women. N Engl J Med 356: 447–458, 2007 - PubMed
-
- Brook RD, Rajagopalan S, Pope CA 3rd, Brook JR, Bhatnagar A, Diez-Roux AV, Holguin F, Hong Y, Luepker RV, Mittleman MA, Peters A, Siscovick D, Smith SC Jr, Whitsel L, Kaufman JD; American Heart Association Council on Epidemiology and Prevention, Council on the Kidney in Cardiovascular Disease, and Council on Nutrition, Physical Activity and Metabolism : Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 121: 2331–2378, 2010 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
