

Confirmed efficacy of etoposide and dexamethasone in HLH treatment: long-term results of the cooperative HLH-2004 study
- PMID: 28935695
- PMCID: PMC5785801
- DOI: 10.1182/blood-2017-06-788349
Confirmed efficacy of etoposide and dexamethasone in HLH treatment: long-term results of the cooperative HLH-2004 study
Abstract
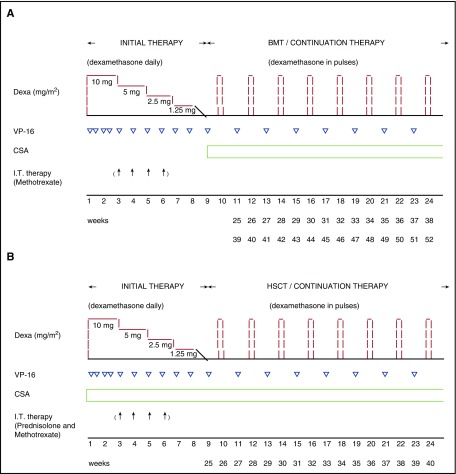
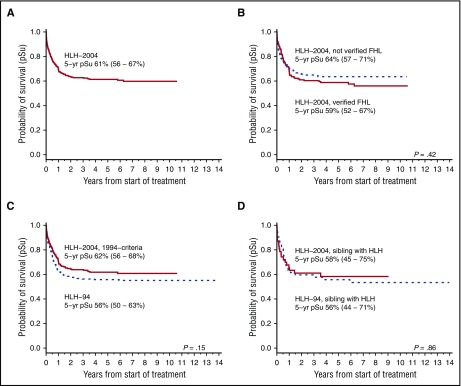
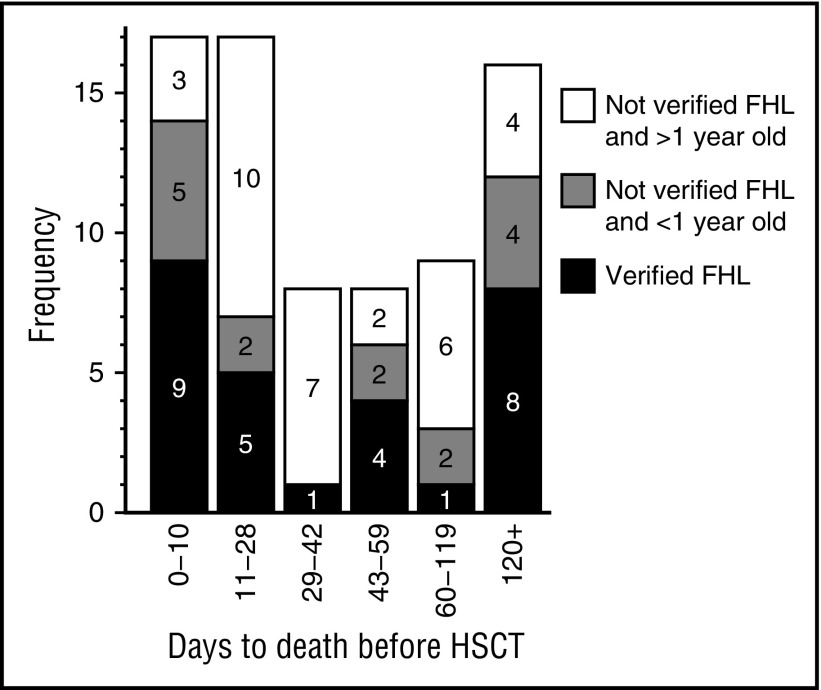
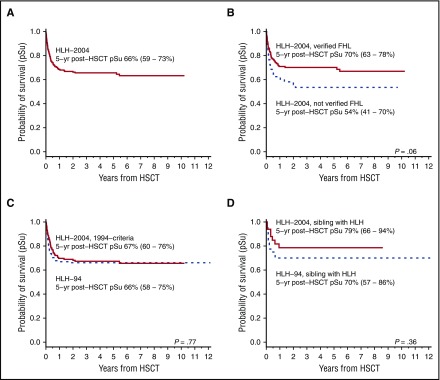
Hemophagocytic lymphohistiocytosis (HLH) is a life-threatening hyperinflammatory syndrome comprising familial/genetic HLH (FHL) and secondary HLH. In the HLH-94 study, with an estimated 5-year probability of survival (pSu) of 54% (95% confidence interval, 48%-60%), systemic therapy included etoposide, dexamethasone, and, from week 9, cyclosporine A (CSA). Hematopoietic stem cell transplantation (HSCT) was indicated in patients with familial/genetic, relapsing, or severe/persistent disease. In HLH-2004, CSA was instead administered upfront, aiming to reduce pre-HSCT mortality and morbidity. From 2004 to 2011, 369 children aged <18 years fulfilled HLH-2004 inclusion criteria (5 of 8 diagnostic criteria, affected siblings, and/or molecular diagnosis in FHL-causative genes). At median follow-up of 5.2 years, 230 of 369 patients (62%) were alive (5-year pSu, 61%; 56%-67%). Five-year pSu in children with (n = 168) and without (n = 201) family history/genetically verified FHL was 59% (52%-67%) and 64% (57%-71%), respectively (familial occurrence [n = 47], 58% [45%-75%]). Comparing with historical data (HLH-94), using HLH-94 inclusion criteria, pre-HSCT mortality was nonsignificantly reduced from 27% to 19% (P = .064 adjusted for age and sex). Time from start of therapy to HSCT was shorter compared with HLH-94 (P =020 adjusted for age and sex) and reported neurological alterations at HSCT were 22% in HLH-94 and 17% in HLH-2004 (using HLH-94 inclusion criteria). Five-year pSu post-HSCT overall was 66% (verified FHL, 70% [63%-78%]). Additional analyses provided specific suggestions on potential pre-HSCT treatment improvements. HLH-2004 confirms that a majority of patients may be rescued by the etoposide/dexamethasone combination but intensification with CSA upfront, adding corticosteroids to intrathecal therapy, and reduced time to HSCT did not improve outcome significantly.
© 2017 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: M.A. and J.-I.H. have been unpaid consultants to NovImmune. The remaining authors declare no competing financial interests.
Figures
Comment in
-
Etoposide for HLH: the limits of efficacy.Blood. 2017 Dec 21;130(25):2692-2693. doi: 10.1182/blood-2017-10-808543. Blood. 2017. PMID: 29269529 No abstract available.
References
-
- Janka GE. Familial hemophagocytic lymphohistiocytosis. Eur J Pediatr. 1983;140(3):221-230. - PubMed
-
- Stepp SE, Dufourcq-Lagelouse R, Le Deist F, et al. . Perforin gene defects in familial hemophagocytic lymphohistiocytosis. Science. 1999;286(5446):1957-1959. - PubMed
-
- Feldmann J, Callebaut I, Raposo G, et al. . Munc13-4 is essential for cytolytic granules fusion and is mutated in a form of familial hemophagocytic lymphohistiocytosis (FHL3). Cell. 2003;115(4):461-473. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
