

Syndromes of Rapidly Progressive Cognitive Decline-Our Experience
- PMID: 28936074
- PMCID: PMC5602264
- DOI: 10.4103/jnrp.jnrp_100_17
Syndromes of Rapidly Progressive Cognitive Decline-Our Experience
Abstract
Background: Dementias are fairly slowly progressive degenerative diseases of brain for which treatment options are very less and carry a lot of burden on family and society. A small percentage of them are rapidly progressive and mostly carry a different course outcome. However, there are no definite criteria other than the time line for these patients.
Aims: The aim of this was to identify and categorize the causes and course of rapidly progressive dementias seen in our center.
Settings and design: Patients who presented with rapid deterioration of cognitive functions within weeks to 1 year between 2011 and December 2016 were evaluated.
Patients and methods: All patients underwent all mandatory tests for dementia including brain imaging. Complete vasculitis workup, autoimmune encephalitis profile including Voltage Gated Potassium Channel, N-methyl-D-aspartic acid receptor, glutamic acid-decarboxylase, thyroid-peroxidase antibody, cerebrospinal fluid, and other special tests such as duodenal biopsy and paraneoplastic workup were done based on clinical indications.
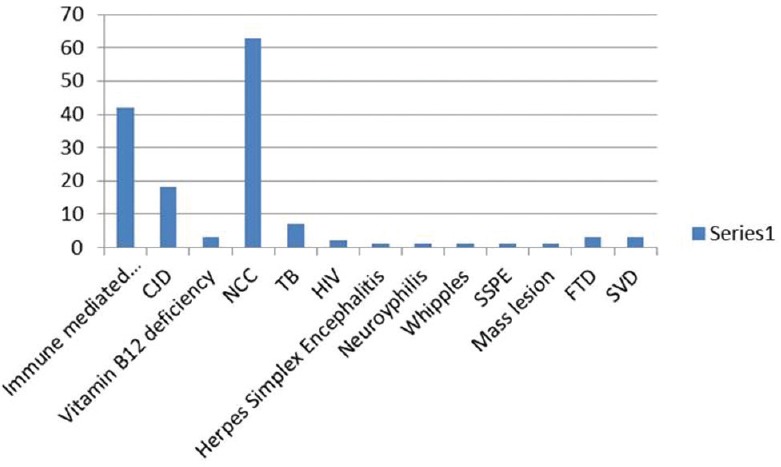
Results and conclusions: Out of 144 patients 42 had immune-mediated encephalopathy, 18 had Creutzfeldt-Jakob disease, 3 had Vitamin B12 deficiency, 63 had infection with neurocysticercosis, 7 had tuberculosis, 2 had HIV, 1 had herpes simplex encephalitis, 1 had neurosyphilis, 1 Whipples disease, 1 had Subacute Sclerosing Panencephalitis, 1 had Mass lesion, 3 had Frontotemporal dementia, and 3 had small vessel disease. Good majority of these patients have infective and immune-mediated causes and less number belong to degenerative group. Therefore, caution is needed to look for treatable cause as it carries a different treatment options and outcome.
Keywords: Degenerations; immune-mediated; infections; nutritional; rapidly progressive dementia.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Roberson ED, Hesse JH, Rose KD, Slama H, Johnson JK, Yaffe K, et al. Frontotemporal dementia progresses to death faster than Alzheimer disease. Neurology. 2005;65:719–25. - PubMed
-
- Becker JT, Farbman ES, Hamilton RL, Lopez OL. Dementia with Lewy bodies. Contemporary Neurobehavioral Syndromes. Joachim, Morris: Selkoe; 2011. pp. 111–29.
-
- Van Everbroeck B, Dobbeleir I, De Waele M, De Deyn P, Martin JJ, Cras P. Differential diagnosis of 201 possible Creutzfeldt-Jakob disease patients. J Neurol. 2004;251:298–304. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources