

Co-stimulation Therapy in Rheumatoid Arthritis: Today and Tomorrow
- PMID: 28936386
- PMCID: PMC5566119
- DOI: 10.1007/s40674-015-0029-0
Co-stimulation Therapy in Rheumatoid Arthritis: Today and Tomorrow
Abstract
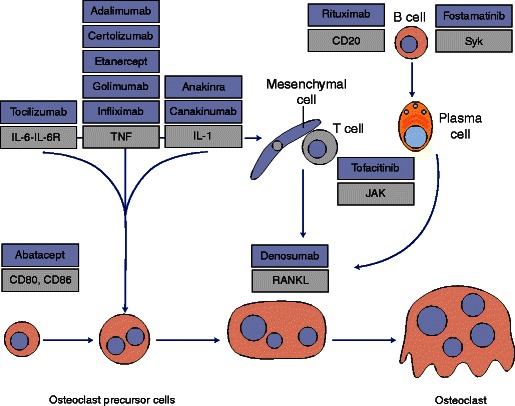
Abatacept is the only T cell co-stimulation modulator approved thus far for the treatment of moderate-to-severe rheumatoid arthritis (RA) and is licensed for use in patients with an inadequate response to methotrexate (MTX) and/or anti-tumor necrosis factor (anti-TNF) therapy. The upstream mechanism of action of abatacept leads to downstream effects in a variety of cell types associated with the production of autoantibodies and pro-inflammatory cytokines implicated in RA. Accumulating data also suggest effects on other cells involved in the pathogenesis of RA, including regulatory T cells and osteoclasts. Clinical trials have demonstrated that abatacept is an effective and well-tolerated treatment in RA. More recently, evidence from the Assessing Very Early Rheumatoid arthritis Treatment (AVERT) trial showed that complete drug-free remission following treatment with abatacept may be a possibility in some patients with early RA, indicating that the disease course could be altered by early intervention. Equivalent efficacy and onset of action of abatacept and anti-TNF therapy have also been demonstrated in patients with an inadequate response to MTX in the Abatacept versus adaliMumab comParison in bioLogic-naïvE rheumatoid arthritis subjects with background methotrexate (AMPLE) trial. Together, these findings support the use of abatacept in early and established RA.
Keywords: Abatacept; CTLA-4-Ig; Co-stimulation; Rheumatoid arthritis; T cell therapy.
Figures


Similar articles
-
Abatacept in biologic-naïve patients and TNF inadequate responders: clinical data in focus.Curr Med Res Opin. 2008 Aug;24(8):2283-94. doi: 10.1185/03007990802223129. Epub 2008 Jun 27. Curr Med Res Opin. 2008. PMID: 18590608 Review.
-
HLA-DRB1 risk alleles for RA are associated with differential clinical responsiveness to abatacept and adalimumab: data from a head-to-head, randomized, single-blind study in autoantibody-positive early RA.Arthritis Res Ther. 2021 Sep 18;23(1):245. doi: 10.1186/s13075-021-02607-7. Arthritis Res Ther. 2021. PMID: 34537057 Free PMC article. Clinical Trial.
-
Greater remission rates in patients with early versus long-standing disease in biologic-naive rheumatoid arthritis patients treated with abatacept: a post hoc analysis of randomized clinical trial data.Clin Exp Rheumatol. 2011 May-Jun;29(3):494-9. Epub 2011 Jun 29. Clin Exp Rheumatol. 2011. PMID: 21722499 Clinical Trial.
-
Attainment and characteristics of clinical remission according to the new ACR-EULAR criteria in abatacept-treated patients with early rheumatoid arthritis: new analyses from the Abatacept study to Gauge Remission and joint damage progression in methotrexate (MTX)-naive patients with Early Erosive rheumatoid arthritis (AGREE).Arthritis Res Ther. 2015 Jun 11;17(1):157. doi: 10.1186/s13075-015-0671-9. Arthritis Res Ther. 2015. PMID: 26063454 Free PMC article. Clinical Trial.
-
Modulation of T-cell co-stimulation in rheumatoid arthritis: clinical experience with abatacept.Clin Drug Investig. 2009;29(3):185-202. doi: 10.2165/00044011-200929030-00005. Clin Drug Investig. 2009. PMID: 19243211 Review.
Cited by
-
Resolution of inflammation during rheumatoid arthritis.Front Cell Dev Biol. 2025 Mar 26;13:1556359. doi: 10.3389/fcell.2025.1556359. eCollection 2025. Front Cell Dev Biol. 2025. PMID: 40206402 Free PMC article. Review.
-
Recent Advances in Understanding the Pathogenesis of Rheumatoid Arthritis: New Treatment Strategies.Cells. 2021 Nov 4;10(11):3017. doi: 10.3390/cells10113017. Cells. 2021. PMID: 34831240 Free PMC article. Review.
-
The Effect of Immunosuppressive Drugs on MDSCs in Transplantation.J Immunol Res. 2018 Jul 3;2018:5414808. doi: 10.1155/2018/5414808. eCollection 2018. J Immunol Res. 2018. PMID: 30057917 Free PMC article. Review.
References
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical