

Chemotherapy for Hepatocellular Carcinoma: Current Evidence and Future Perspectives
- PMID: 28936405
- PMCID: PMC5606970
- DOI: 10.14218/JCTH.2017.00002
Chemotherapy for Hepatocellular Carcinoma: Current Evidence and Future Perspectives
Abstract
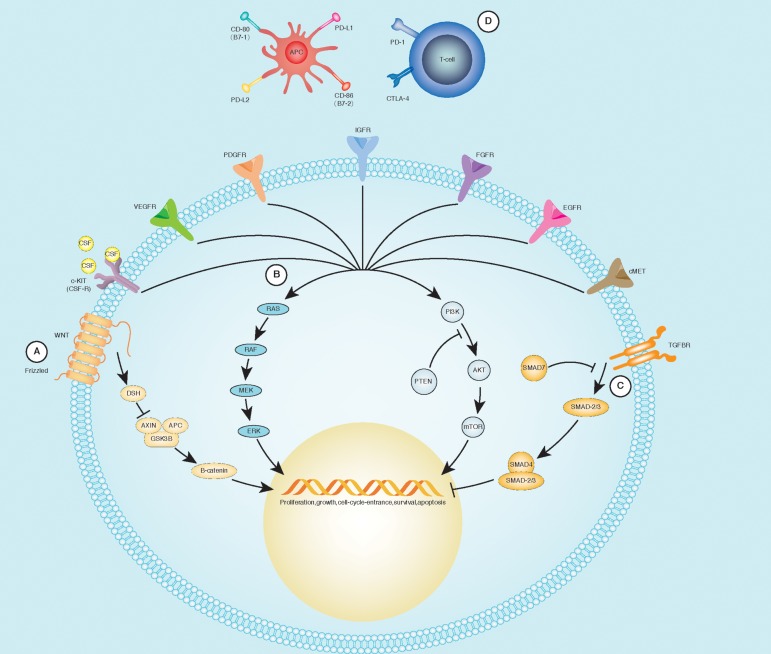
Hepatocarcinogenesis is a multistep process, heralded by abnormalities in cell differentiation and proliferation and sustained by an aberrant neoangiogenesis. Understanding the underlying molecular pathogenesis leading to hepatocellular carcinoma is a prerequisite to develop new drugs that will hamper or block the steps of these pathways. As hepatocellular carcinoma has higher arterial vascularization than normal liver, this could be a good target for novel molecular therapies. Introduction of the antiangiogenic drug sorafenib into clinical practice since 2008 has led to new perspectives in the management of this tumor. The importance of this drug lies not only in the modest gain of patients' survival, but in having opened a roadmap towards the development of new molecules and targets. Unfortunately, after the introduction of sorafenib, during the last years, a wide number of clinical trials on antiangiogenic therapies failed in achieving significant results. However, many of these trials are still ongoing and promise to improve overall survival and progression-free survival. A recent clinical trial has proven regorafenib effective in patients showing tumor progression under sorafenib, thus opening new interesting therapeutic perspectives. Many other expectations have been borne from the discovery of the immune checkpoint blockade, already known in other solid malignancies. Furthermore, a potential role in hepatocellular carcinoma therapy may derive from the use of branched-chain amino acids and of nutritional support. This review analyses the biomolecular pathways of hepatocellular carcinoma and the ongoing studies, the actual evidence and the future perspectives concerning drug therapy in this open field.
Keywords: Branched-chain amino acids; Hepatocellular carcinoma; Immunotherapy; Molecular target therapies.
Conflict of interest statement
The authors have no conflict of interests related to this publication.
Figures
Similar articles
-
Strategies to Improve the Antitumor Effect of Immunotherapy for Hepatocellular Carcinoma.Front Immunol. 2021 Nov 26;12:783236. doi: 10.3389/fimmu.2021.783236. eCollection 2021. Front Immunol. 2021. PMID: 34899747 Free PMC article. Review.
-
Selective internal radiation therapies for unresectable early-, intermediate- or advanced-stage hepatocellular carcinoma: systematic review, network meta-analysis and economic evaluation.Health Technol Assess. 2020 Sep;24(48):1-264. doi: 10.3310/hta24480. Health Technol Assess. 2020. PMID: 33001024 Free PMC article.
-
Systemic treatments for hepatocellular carcinoma: challenges and future perspectives.Hepat Oncol. 2018 Feb 8;5(1):HEP01. doi: 10.2217/hep-2017-0020. eCollection 2018 Jan. Hepat Oncol. 2018. PMID: 30302192 Free PMC article. Review.
-
Chemotherapy for hepatocellular carcinoma: current status and future perspectives.Jpn J Clin Oncol. 2018 Feb 1;48(2):103-114. doi: 10.1093/jjco/hyx180. Jpn J Clin Oncol. 2018. PMID: 29253194 Review.
-
Role of immunotherapy in the management of hepatocellular carcinoma: current standards and future directions.Curr Oncol. 2020 Nov;27(Suppl 3):S152-S164. doi: 10.3747/co.27.7315. Epub 2020 Nov 1. Curr Oncol. 2020. PMID: 33343209 Free PMC article. Review.
Cited by
-
Skeletal Muscle Loss during Multikinase Inhibitors Therapy: Molecular Pathways, Clinical Implications, and Nutritional Challenges.Nutrients. 2020 Oct 12;12(10):3101. doi: 10.3390/nu12103101. Nutrients. 2020. PMID: 33053632 Free PMC article. Review.
-
Targeting Yes1 Associated Transcriptional Regulator Inhibits Hepatocellular Carcinoma Progression and Improves Sensitivity to Sorafenib: An in vitro and in vivo Study.Onco Targets Ther. 2020 Oct 29;13:11071-11087. doi: 10.2147/OTT.S249412. eCollection 2020. Onco Targets Ther. 2020. PMID: 33149619 Free PMC article.
-
Bioinformatic Deconstruction of Differentially Expressed Sequence Tags in Hepatocellular Carcinoma Based on Artificial Neural Network.Contrast Media Mol Imaging. 2022 Oct 10;2022:6716324. doi: 10.1155/2022/6716324. eCollection 2022. Contrast Media Mol Imaging. 2022. Retraction in: Contrast Media Mol Imaging. 2023 Nov 29;2023:9797605. doi: 10.1155/2023/9797605. PMID: 36299828 Free PMC article. Retracted.
-
IFI44L is a novel tumor suppressor in human hepatocellular carcinoma affecting cancer stemness, metastasis, and drug resistance via regulating met/Src signaling pathway.BMC Cancer. 2018 May 30;18(1):609. doi: 10.1186/s12885-018-4529-9. BMC Cancer. 2018. PMID: 29848298 Free PMC article.
-
A novel oncolytic adenovirus inhibits hepatocellular carcinoma growth.J Zhejiang Univ Sci B. 2019 Dec.;20(12):1003-1013. doi: 10.1631/jzus.B1900089. J Zhejiang Univ Sci B. 2019. PMID: 31749347 Free PMC article.
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. doi:10.1002/ijc.29210. - DOI - PubMed
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. doi:10.3322/canjclin.55.2.74. - DOI - PubMed
-
- Tanaka H, Imai Y, Hiramatsu N, Ito Y, Imanaka K, Oshita M, et al. Declining incidence of hepatocellular carcinoma in Osaka, Japan, from 1990 to 2003. Ann Intern Med. 2008;148:820–826. doi:10.7326/0003-4819-148-11-200806030-00004. - DOI - PubMed
-
- Bosetti C, Levi F, Boffetta P, Lucchini F, Negri E, La Vecchia C. Trends in mortality from hepatocellular carcinoma in Europe, 1980–2004. Hepatology. 2008;48:137–145. doi:10.1002/hep.22312. - DOI - PubMed
-
- Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet. 2003;362:1907–1917. doi:10.1016/S0140-6736(03)14964-1. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials