

Development and Standardization of a New Cognitive Assessment Test Battery for Chinese Aphasic Patients: A Preliminary Study
- PMID: 28937032
- PMCID: PMC5634076
- DOI: 10.4103/0366-6999.215326
Development and Standardization of a New Cognitive Assessment Test Battery for Chinese Aphasic Patients: A Preliminary Study
Abstract
Background: Nonlinguistic cognitive impairment has become an important issue for aphasic patients, but currently there are few neuropsychological cognitive assessment tests for it. To get more information on cognitive impairment of aphasic patients, this study aimed to develop a new cognitive assessment test battery for aphasic patients, the Non-language-based Cognitive Assessment (NLCA), and evaluate its utility in Chinese-speaking patients with aphasia.
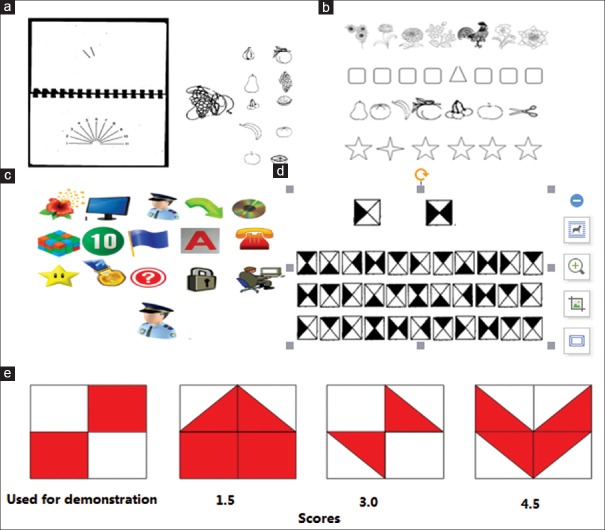
Methods: The NLCA consists of five nonverbal tests, which could assess five nonlinguistic cognitive domains such as visuospatial functions, attention test, memory, reasoning, and executive functions of aphasic patients. All tests are modified from the nonverbal items of the current existed tests with some changes to the characteristics of Chinese culture. The NLCA was tested in 157 participants (including 57 aphasic patients, 50 mild cognitive impairment (MCI) patients, and 50 normal controls), and was compared with other well-established relative neuropsychological tests on the reliability, validity, and utility.
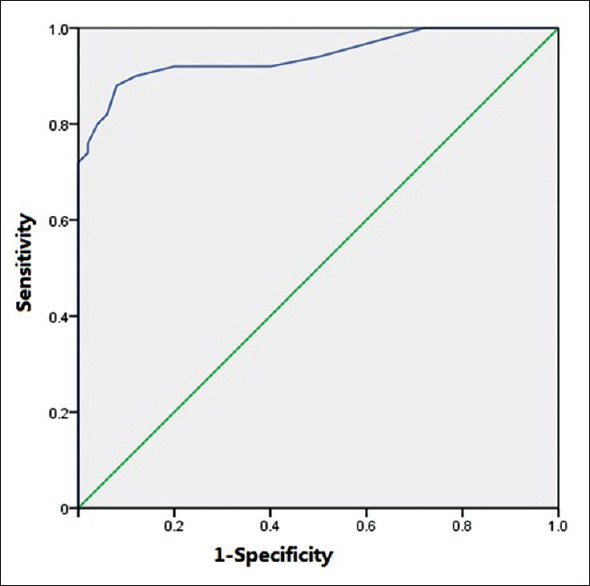
Results: The NLCA was fully applicable in the MCI patients and the normal controls, almost working in the aphasic patients (57/62 patients, 91.9%). The NLCA scores were 66.70 ± 6.30, 48.67 ± 15.04, and 77.58 ± 2.56 for the MCI group, the aphasic group, and the control group, respectively , and a significant difference was found among three groups (F = 118.446, P < 0.001). The Cronbach's alpha of the NLCA as an index of internal consistency was 0.805, and the test-retest and interrater reliability was adequate (r=0.977 and r= 0.970, respectively). The correlations of the cognitive subtests and their validation instruments were between 0.540 and 0.670 (all P < 0.05). Spearman's correlation analysis indicated that the coefficient of internal consistency of each subtest itself was higher than other subtests. When choosing the Montreal Cognitive Assessment score of <26 as the diagnostic criteria of cognitive impairment, the area under the curve for all participants in the control and MCI groups was 0.942 (95% confidence interval: 0.895-0.989), and an optimal cutoff point of 75.00 seemed to provide the best balance between sensitivity and specificity. Age (r = -0.406, P < 0.001) was the main influence factor for the NLCA.
Conclusions: The NLCA could efficiently differentiate the cognitive impairment patients from the normal controls and is a reliable and valid cognitive assessment test battery to specially find nonlinguistic cognitive function for aphasic patients.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
A new test battery to assess aphasic disturbances and associated cognitive dysfunctions -- German normative data on the aphasia check list.J Clin Exp Neuropsychol. 2005 Oct;27(7):779-94. doi: 10.1080/13803390490918273. J Clin Exp Neuropsychol. 2005. PMID: 16183613
-
Validity of the Cantonese Chinese Montreal Cognitive Assessment in Southern Chinese.Geriatr Gerontol Int. 2015 Jan;15(1):96-103. doi: 10.1111/ggi.12237. Epub 2014 Jan 24. Geriatr Gerontol Int. 2015. PMID: 24456109
-
Limitations for interpreting failure on individual subtests of the Montreal Cognitive Assessment.J Geriatr Psychiatry Neurol. 2013 Mar;26(1):19-28. doi: 10.1177/0891988712473802. Epub 2013 Feb 4. J Geriatr Psychiatry Neurol. 2013. PMID: 23385364
-
Cross-sectional associations between metabolic syndrome and performance across cognitive domains: A systematic review.Appl Neuropsychol Adult. 2019 Mar-Apr;26(2):186-199. doi: 10.1080/23279095.2017.1363039. Epub 2017 Sep 25. Appl Neuropsychol Adult. 2019. PMID: 28945138
-
A meta-analysis of executive dysfunction in patients with schizophrenia: Different degree of impairment in the ecological subdomains of the Behavioural Assessment of the Dysexecutive Syndrome.Psychiatry Res. 2019 Feb;272:230-236. doi: 10.1016/j.psychres.2018.12.088. Epub 2018 Dec 20. Psychiatry Res. 2019. PMID: 30590277
Cited by
-
Capturing Neuroplastic Changes after iTBS in Patients with Post-Stroke Aphasia: A Pilot fMRI Study.Brain Sci. 2021 Oct 31;11(11):1451. doi: 10.3390/brainsci11111451. Brain Sci. 2021. PMID: 34827450 Free PMC article.
-
Naming difficulties after thyroid stimulating hormone suppression therapy in patients with differentiated thyroid carcinoma: a prospective cohort study.Endocrine. 2019 Aug;65(2):327-337. doi: 10.1007/s12020-019-01943-8. Epub 2019 May 5. Endocrine. 2019. PMID: 31056722 Free PMC article.
-
Language reorganization patterns in global aphasia-evidence from fNIRS.Front Neurol. 2023 Jan 6;13:1025384. doi: 10.3389/fneur.2022.1025384. eCollection 2022. Front Neurol. 2023. PMID: 36686505 Free PMC article.
-
A physician survey of poststroke aphasia diagnosis and treatment in China: SPEECH study.Medicine (Baltimore). 2021 Jun 4;100(22):e25833. doi: 10.1097/MD.0000000000025833. Medicine (Baltimore). 2021. PMID: 34087826 Free PMC article.
-
Effects of low-frequency rTMS combined with speech and language therapy on Broca's aphasia in subacute stroke patients.Front Neurol. 2024 Oct 30;15:1473254. doi: 10.3389/fneur.2024.1473254. eCollection 2024. Front Neurol. 2024. PMID: 39539660 Free PMC article.
References
-
- Bonini MV, Radanovic M. Cognitive deficits in post-stroke aphasia. Arq Neuropsiquiatr. 2015;73:840–7. doi: 10.1590/0004-282X20150133. - PubMed
-
- Yu ZZ, Jiang SJ, Bi S, Li J, Lei D, Sun LL. Relationship between linguistic functions and cognitive functions in a clinical study of Chinese patients with post-stroke aphasia. Chin Med J. 2013;126:1252–6. doi: 10.3760/cma.j.issn.0366-6999.20121463. - PubMed
-
- Seniów J, Litwin M, Lesniak M. The relationship between non-linguistic cognitive deficits and language recovery in patients with aphasia. J Neurol Sci. 2009;283:91–4. doi: 10.1016/j.jns.2009.02.315. - PubMed
-
- Murray LL. Attention and other cognitive deficits in aphasia: Presence and relation to language and communication measures. Am J Speech Lang Pathol. 2012;21:S51–64. doi: 10.1044/1058-0360(2012/11-0067) - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
