

Bariatric Surgery and the Risk of Cancer in a Large Multisite Cohort
- PMID: 28938270
- PMCID: PMC6201282
- DOI: 10.1097/SLA.0000000000002525
Bariatric Surgery and the Risk of Cancer in a Large Multisite Cohort
Abstract
Objective: To determine whether bariatric surgery is associated with a lower risk of cancer.
Background: Obesity is strongly associated with many types of cancer. Few studies have examined the relationship between bariatric surgery and cancer risk.
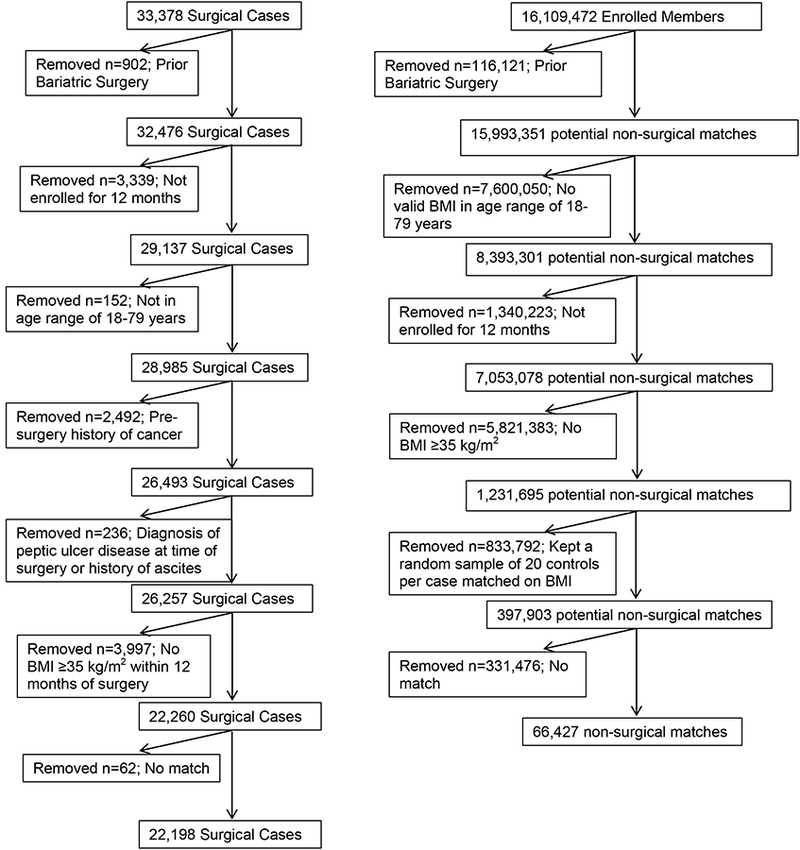
Methods: We conducted a retrospective cohort study of patients undergoing bariatric surgery between 2005 and 2012 with follow-up through 2014 using data from a large integrated health insurance and care delivery systems with 5 study sites. The study included 22,198 subjects who had bariatric surgery and 66,427 nonsurgical subjects matched on sex, age, study site, body mass index, and Elixhauser comorbidity index. Multivariable Cox proportional-hazards models were used to examine incident cancer up to 10 years after bariatric surgery compared to the matched nonsurgical patients.
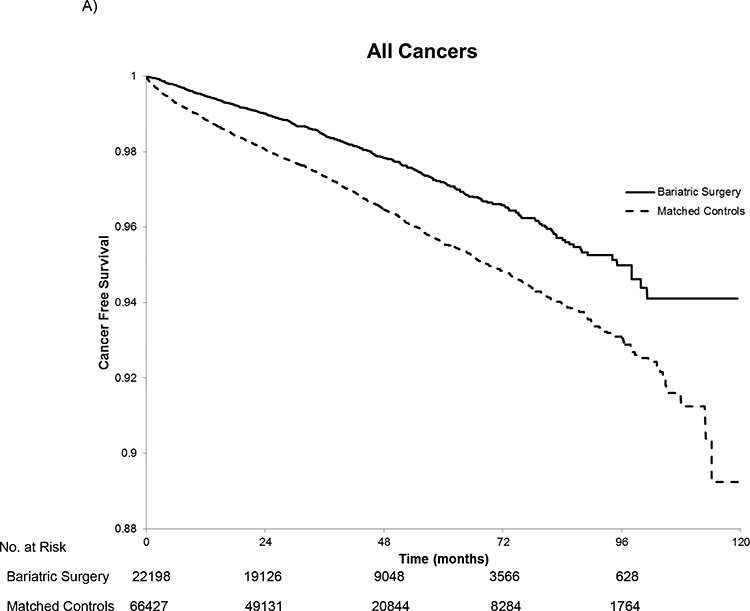
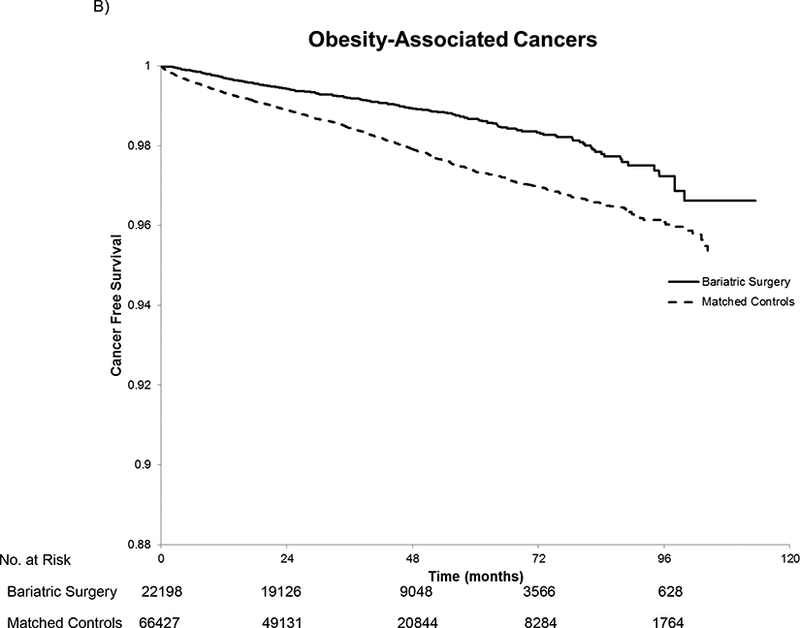
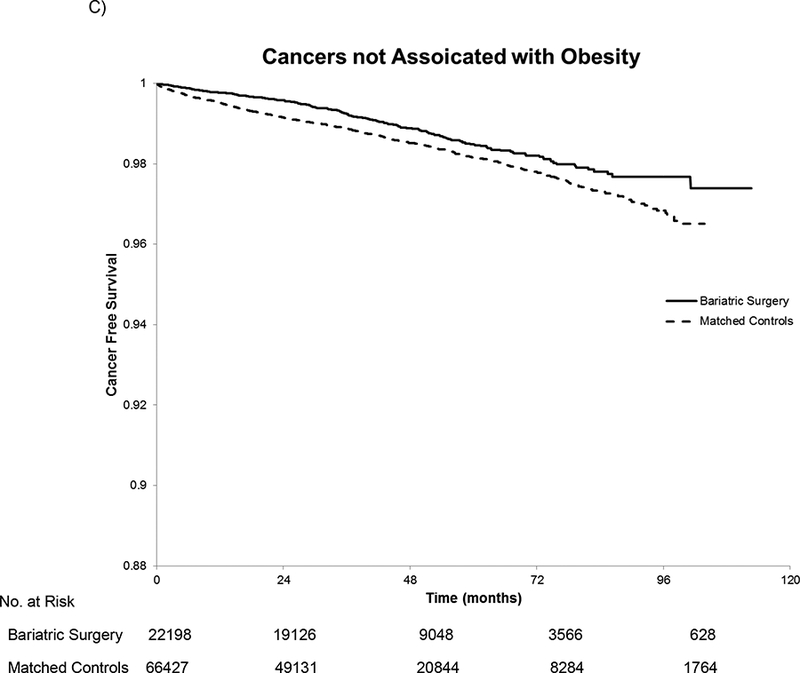
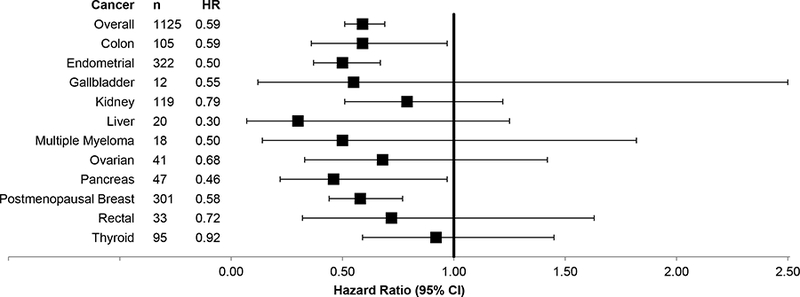
Results: After a mean follow-up of 3.5 years, we identified 2543 incident cancers. Patients undergoing bariatric surgery had a 33% lower hazard of developing any cancer during follow-up [hazard ratio (HR) 0.67, 95% confidence interval (CI) 0.60, 0.74, P < 0.001) compared with matched patients with severe obesity who did not undergo bariatric surgery, and results were even stronger when the outcome was restricted to obesity-associated cancers (HR 0.59, 95% CI 0.51, 0.69, P < 0.001). Among the obesity-associated cancers, the risk of postmenopausal breast cancer (HR 0.58, 95% CI 0.44, 0.77, P < 0.001), colon cancer (HR 0.59, 95% CI 0.36, 0.97, P = 0.04), endometrial cancer (HR 0.50, 95% CI 0.37, 0.67, P < 0.001), and pancreatic cancer (HR 0.46, 95% CI 0.22, 0.97, P = 0.04) was each statistically significantly lower among those who had undergone bariatric surgery compared with matched nonsurgical patients.
Conclusions: In this large, multisite cohort of patients with severe obesity, bariatric surgery was associated with a lower risk of incident cancer, particularly obesity-associated cancers, such as postmenopausal breast cancer, endometrial cancer, and colon cancer. More research is needed to clarify the specific mechanisms through which bariatric surgery lowers cancer risk.
Conflict of interest statement
Conflicts of Interests:
No conflicts of interest to declare.
Figures
Comment in
-
Cancer risk after bariatric surgery - is colorectal cancer a special case?Nat Rev Gastroenterol Hepatol. 2018 Nov;15(11):653-654. doi: 10.1038/s41575-018-0070-1. Nat Rev Gastroenterol Hepatol. 2018. PMID: 30267023 No abstract available.
Similar articles
-
Association of Bariatric Surgery With Cancer Risk and Mortality in Adults With Obesity.JAMA. 2022 Jun 28;327(24):2423-2433. doi: 10.1001/jama.2022.9009. JAMA. 2022. PMID: 35657620 Free PMC article.
-
Association Between Weight Loss and the Risk of Cancer after Bariatric Surgery.Obesity (Silver Spring). 2017 Nov;25 Suppl 2(Suppl 2):S52-S57. doi: 10.1002/oby.22002. Obesity (Silver Spring). 2017. PMID: 29086527 Free PMC article.
-
Microvascular Outcomes in Patients With Diabetes After Bariatric Surgery Versus Usual Care: A Matched Cohort Study.Ann Intern Med. 2018 Sep 4;169(5):300-310. doi: 10.7326/M17-2383. Epub 2018 Aug 7. Ann Intern Med. 2018. PMID: 30083761 Free PMC article.
-
Review of the key results from the Swedish Obese Subjects (SOS) trial - a prospective controlled intervention study of bariatric surgery.J Intern Med. 2013 Mar;273(3):219-34. doi: 10.1111/joim.12012. Epub 2013 Feb 8. J Intern Med. 2013. PMID: 23163728 Review.
-
Incidence of cancer for patients after bariatric surgery: evidence from 33 cohort studies.Surg Obes Relat Dis. 2024 May;20(5):467-481. doi: 10.1016/j.soard.2023.11.010. Epub 2023 Nov 27. Surg Obes Relat Dis. 2024. PMID: 38151417
Cited by
-
Obesity and Breast Cancer: A Case of Inflamed Adipose Tissue.Cancers (Basel). 2020 Jun 25;12(6):1686. doi: 10.3390/cancers12061686. Cancers (Basel). 2020. PMID: 32630445 Free PMC article. Review.
-
Obesity, cancer risk, and time-restricted eating.Cancer Metastasis Rev. 2022 Sep;41(3):697-717. doi: 10.1007/s10555-022-10061-3. Epub 2022 Aug 19. Cancer Metastasis Rev. 2022. PMID: 35984550 Free PMC article. Review.
-
Obesity Surgery and Cancer: What Are the Unanswered Questions?Front Endocrinol (Lausanne). 2020 Apr 15;11:213. doi: 10.3389/fendo.2020.00213. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32351453 Free PMC article. Review.
-
THE GROWING EVIDENCE OF THE RELATIONSHIP BETWEEN OBESITY AND CANCER AND THE ROLE OF BARIATRIC SURGERY.Arq Bras Cir Dig. 2024 Dec 2;37:e1838. doi: 10.1590/0102-6720202400044e1838. eCollection 2024. Arq Bras Cir Dig. 2024. PMID: 39630839 Free PMC article. Review.
-
The Effectiveness of Metabolic Bariatric Surgery in Preventing Gynecologic Cancer - from Pathophysiology to Clinical Outcomes.J Cancer. 2024 Jan 1;15(4):1077-1092. doi: 10.7150/jca.91471. eCollection 2024. J Cancer. 2024. PMID: 38230225 Free PMC article. Review.
References
-
- Polednak AP. Estimating the number of U.S. incident cancers attributable to obesity and the impact on temporal trends in incidence rates for obesity-related cancers. Cancer Detect Prev 2008;32:190–9. - PubMed
-
- Calle EE, Rodriguez C, Walker-Thurmond K, et al. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 2003;348:1625–38. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
