

Autosomal Dominant Hyper-IgE Syndrome in the USIDNET Registry
- PMID: 28939137
- PMCID: PMC5858974
- DOI: 10.1016/j.jaip.2017.06.041
Autosomal Dominant Hyper-IgE Syndrome in the USIDNET Registry
Abstract
Background: Autosomal dominant hyper-IgE syndrome (AD-HIES) is a rare condition.
Objective: Data from the USIDNET Registry provide a resource to examine the characteristics of patients with rare immune deficiency diseases.
Methods: A query was submitted to the USIDNET requesting deidentified data for patients with physician-diagnosed AD-HIES through July 2016.
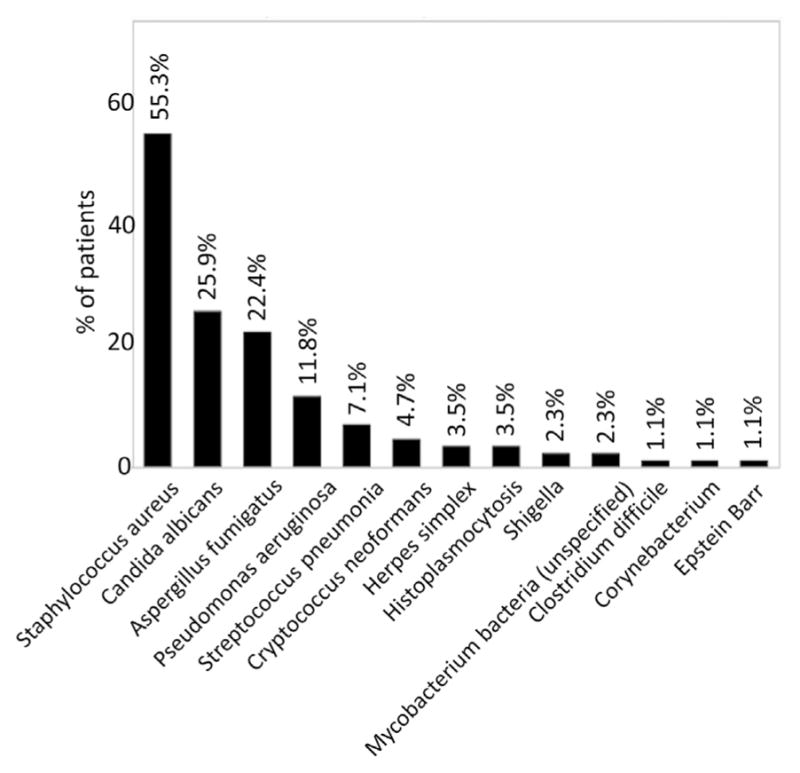
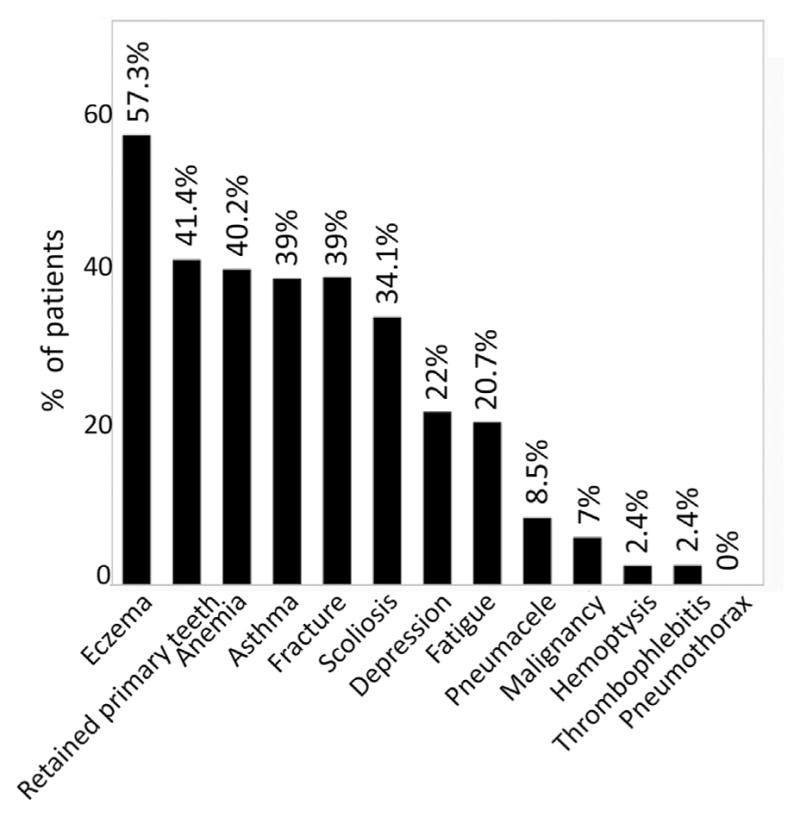
Results: Data on 85 patients diagnosed with AD-HIES (50 males; 35 females) born between 1950 and 2013, collected by 14 physicians from 25 states and Quebec, were entered into the USIDNET Registry by July 2016. Cumulative follow-up was 2157 years. Of these patients, 45.9% had a family history of HIES. The complications reported included skin abscesses (74.4%), eczema (57.7%), retained primary teeth (41.4%), fractures (39%), scoliosis (34.1%), and cancer (7%). Reported allergic diseases included food (37.8%), environmental (18%), and drugs (42.7%). The mean serum IgE level was 8383.7 kU/mL and was inversely correlated to the patient's age. A total of 49.4% had eosinophilia; 56% were known to be on trimethoprim-sulfamethoxazole, 26.6% on antifungal coverage, and 30.6% on immunoglobulin replacement therapy. Pneumonias were more commonly attributed to Staphylococcus aureus (55.3%) or Aspergillus fumigatus (22.4%); 19.5% had a history of lung abscess; these were most often associated with Pseudomonas aeruginosa (P Fisher's exact test = .029) or A. fumigatus (P Fisher's exact test = .016). Lung abscesses were significantly associated with drug reactions (P χ2 = .01; odds ratio: 4.03 [1.2-12.97]), depression (P Fisher's exact test = .036), and lower Karnofsky index scores (P Mann-Whitney = .007).
Discussion: Data from the USIDNET Registry summarize the currently reported clinical characteristics of a large cohort of subjects with AD-HIES.
Keywords: Buckley-Job syndrome; Chronic mucocutaneous candidiasis; Immunodeficiency; Pneumatocele; Quality of life.
Copyright © 2017 American Academy of Allergy, Asthma & Immunology. All rights reserved.
Conflict of interest statement
Conflicts of interest: J. M. Puck has received research support from the National Institutes of Health (National Institute of Allergy and Infectious Disease US Immune Deficiency Network [USIDNet] U24 subcontract); receives royalties from UpToDate and Oxford U Press; spouse is employed by and has stock options in Invitae. K. E. Sullivan is on the boards for the American Academy of Allergy, Asthma, and Immunology (AAAAI) and Immune Deficiency Foundation (IDF); is employed by the Children’s Hospital of Philadelphia; has received travel support from the AAAAI, European Society for Immune Deficiency, and Clinical Immunology Society. R. Buckley is employed by Duke University Medical Center. E. Haddad has received consultancy fees from Leadiant; and has received research support from CSL Behring. H. D. Ochs is on the Grifols Advisory Board. R. Fuleihan has received consultancy and lecture fees from Shire. J. Routes has received support on symposia (including travel) from CSL Behring. C. Cunningham-Rundles has received research support from IDF and USIDNet. The rest of the authors declare that they have no relevant conflicts of interest.
Figures

References
-
- Davis SD, Schaller J, Wedgwood RJ. Job’s syndrome. Recurrent, “cold”, staphylococcal abscesses. Lancet. 1966;1:1013–5. - PubMed
-
- Buckley RH, Wray BB, Belmaker EZ. Extreme hyperimmunoglobulinemia E and undue susceptibility to infection. Pediatrics. 1972;49:59–70. - PubMed
-
- Grimbacher B, Holland SM, Gallin JI, Greenberg F, Hill SC, Malech HL, et al. Hyper-IgE syndrome with recurrent infections—an autosomal dominant multi-system disorder. N Engl J Med. 1999;340:692–702. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
