

Genetic loci of Staphylococcus aureus associated with anti-neutrophil cytoplasmic autoantibody (ANCA)-associated vasculitides
- PMID: 28939882
- PMCID: PMC5610336
- DOI: 10.1038/s41598-017-12450-z
Genetic loci of Staphylococcus aureus associated with anti-neutrophil cytoplasmic autoantibody (ANCA)-associated vasculitides
Abstract
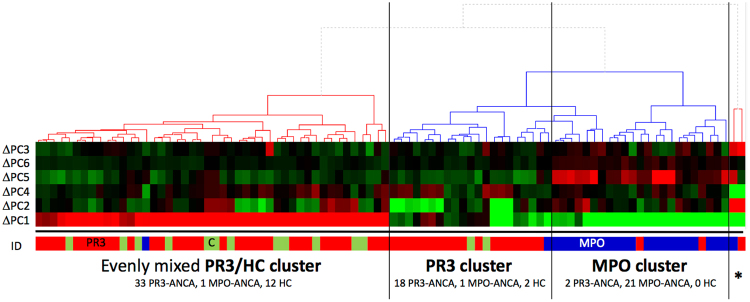
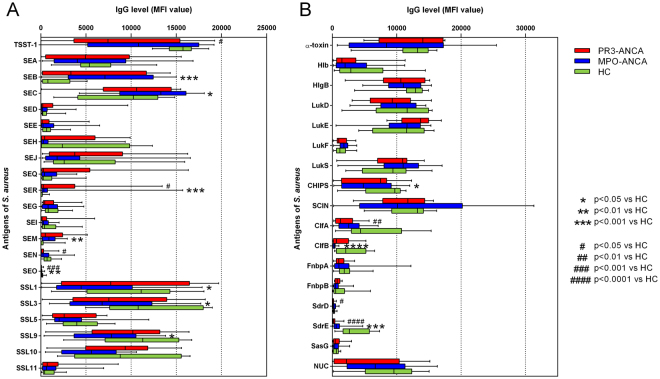
The proteinase 3 (PR3)-positive anti-neutrophil cytoplasmic autoantibody (ANCA)-associated vasculitis (AAV) granulomatosis with polyangiitis (GPA) has been associated with chronic nasal S. aureus carriage, which is a risk factor for disease relapse. The present study was aimed at comparing the genetic make-up of S. aureus isolates from PR3-ANCA-positive GPA patients with that of isolates from patients suffering from myeloperoxidase (MPO)-ANCA-positive AAV, and isolates from healthy controls. Based on a DNA microarray-based approach, we show that not only PR3-ANCA-positive GPA patients, but also MPO-ANCA-positive AAV patients mainly carried S. aureus types that are prevalent in the general population. Nonetheless, our data suggests that MPO-ANCA-associated S. aureus isolates may be distinct from healthy control- and PR3-ANCA-associated isolates. Furthermore, several genetic loci of S. aureus are associated with either PR3-ANCA- or MPO-ANCA-positive AAV, indicating a possible role for pore-forming toxins, such as leukocidins, in PR3-ANCA-positive GPA. Contrary to previous studies, no association between AAV and superantigens was detected. Our findings also show that a lowered humoral immune response to S. aureus is common for PR3-ANCA- and MPO-ANCA-positive AAV. Altogether, our observations imply that the presence or absence of particular virulence genes of S. aureus isolates from AAV patients contributes to disease progression and/or relapse.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
