

Quantitative analysis of the effect of end-tidal carbon dioxide on regional cerebral oxygen saturation in patients undergoing carotid endarterectomy under general anaesthesia
- PMID: 28940441
- PMCID: PMC5777433
- DOI: 10.1111/bcp.13441
Quantitative analysis of the effect of end-tidal carbon dioxide on regional cerebral oxygen saturation in patients undergoing carotid endarterectomy under general anaesthesia
Abstract
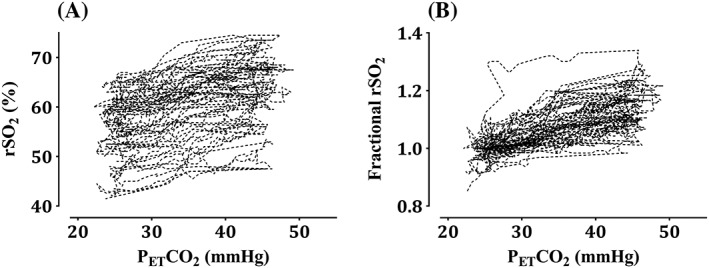
Aims: Regional cerebral oxygen saturation (rSO2 ) is currently the most used measure in clinical practice to monitor cerebral ischaemia in patients undergoing carotid endarterectomy (CEA). Although end-tidal carbon dioxide (PET CO2 ) is known as a factor that influences rSO2 , the relationship between PET CO2 and rSO2 has not been quantitatively evaluated in patients with severe arteriosclerosis. This study aimed to evaluate the effect of PET CO2 on rSO2 in patients undergoing CEA under general anaesthesia.
Methods: The intervention to change PET CO2 was conducted between skin incision and clamping of the carotid artery. The rSO2 values were observed by changing PET CO2 in the range of 25-45 mmHg. The PET CO2 -rSO2 relationship was characterized by population analysis using a turnover model.
Results: In total, 1651 rSO2 data points from 30 patients were used to determine the pharmacodynamic characteristics. Hypertension (HTN) and systolic blood pressure (SBP) were significant covariates on the slope factor in the stimulatory effect of PET CO2 on rSO2 and fractional turnover rate constant (kout ), respectively. The estimates of the parameters were kout (min-1 ): 3.59 for SBP <90 mmHg and 0.491 for SBP ≥90 mmHg, slope: 0.00321 for patients with HTN and 0.00664 for patients without HTN.
Conclusion: The presence of HTNattenuates the response of rSO2 after a change in PET CO2 . When cerebral blood flow is in a state of decline caused by a decrease in SBP to <90 mmHg, the response of rSO2 to PET CO2 is increased. It is advisable to maintain SBP >90 mmHg in patients with HTNduring CEA.
Keywords: pharmacodynamics; satherosclerosis; vascular disease.
© 2017 The British Pharmacological Society.
Figures



Similar articles
-
Cerebral oxygenation and processed EEG response to clamping and shunting during carotid endarterectomy under general anesthesia.J Clin Monit Comput. 2015 Dec;29(6):713-20. doi: 10.1007/s10877-014-9657-4. Epub 2015 Jan 9. J Clin Monit Comput. 2015. PMID: 25572653
-
Non-Invasive Cerebral Autoregulation Monitoring During Awake Carotid Endarterectomy Identifies Clinically Significant Brain Ischaemia.Eur J Vasc Endovasc Surg. 2020 Nov;60(5):647-654. doi: 10.1016/j.ejvs.2020.07.076. Epub 2020 Aug 17. Eur J Vasc Endovasc Surg. 2020. PMID: 32819817
-
Near Infrared Spectroscopy as a Predictor for Shunt Requirement During Carotid Endarterectomy.Eur J Vasc Endovasc Surg. 2017 Jun;53(6):783-791. doi: 10.1016/j.ejvs.2017.02.033. Epub 2017 Apr 19. Eur J Vasc Endovasc Surg. 2017. PMID: 28431821
-
The Diagnostic Accuracy of Intra-Operative Near Infrared Spectroscopy in Carotid Artery Endarterectomy Under Regional Anaesthesia: Systematic Review and Meta-Analysis.Eur J Vasc Endovasc Surg. 2021 Oct;62(4):522-531. doi: 10.1016/j.ejvs.2021.05.042. Epub 2021 Jul 17. Eur J Vasc Endovasc Surg. 2021. PMID: 34284934
-
The value of near-infrared spectroscopy measured cerebral oximetry during carotid endarterectomy in perioperative stroke prevention. A review.Eur J Vasc Endovasc Surg. 2009 Nov;38(5):539-45. doi: 10.1016/j.ejvs.2009.07.008. Epub 2009 Aug 7. Eur J Vasc Endovasc Surg. 2009. PMID: 19665397 Review.
Cited by
-
Accuracy assessment of a PION TCI pump based on international standards.Anesth Pain Med (Seoul). 2019 Oct 31;14(4):407-411. doi: 10.17085/apm.2019.14.4.407. Anesth Pain Med (Seoul). 2019. PMID: 33329769 Free PMC article.
-
Effect of hemoglobin content on cerebral oxygen saturation during surgery for scoliosis in pediatric patients.BMC Anesthesiol. 2021 Jun 1;21(1):165. doi: 10.1186/s12871-021-01382-x. BMC Anesthesiol. 2021. PMID: 34074238 Free PMC article.
-
Quantitative analysis of the effect of fraction of inspired oxygen on peripheral oxygen saturation in healthy volunteers.J Dent Anesth Pain Med. 2020 Apr;20(2):73-81. doi: 10.17245/jdapm.2020.20.2.73. Epub 2020 Apr 27. J Dent Anesth Pain Med. 2020. PMID: 32395612 Free PMC article.
-
A pharmacodynamic model of tidal volume and inspiratory sevoflurane concentration in children during spontaneous breathing.J Pharmacokinet Pharmacodyn. 2021 Apr;48(2):253-259. doi: 10.1007/s10928-020-09729-6. Epub 2021 Jan 2. J Pharmacokinet Pharmacodyn. 2021. PMID: 33387166
References
-
- Eckstein HH, Ringleb P, Allenberg JR, Berger J, Fraedrich G, Hacke W, et al Results of the Stent‐Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol 2008; 7: 893–902. - PubMed
-
- Choi BM, Park SK, Shin S, Cho YP, Kwon TW, Choi YJ, et al Neurologic derangement and regional cerebral oxygen desaturation associated with patency of the circle of Willis during carotid endarterectomy. J Cardiothorac Vasc Anesth 2015; 29: 1200–1205. - PubMed
-
- Pennekamp CW, Moll FL, de Borst GJ. The potential benefits and the role of cerebral monitoring in carotid endarterectomy. Curr Opin Anaesthesiol 2011; 24: 693–697. - PubMed
-
- Samra SK, Dy EA, Welch K, Dorje P, Zelenock GB, Stanley JC. Evaluation of a cerebral oximeter as a monitor of cerebral ischemia during carotid endarterectomy. Anesthesiology 2000; 93: 964–970. - PubMed
-
- Mille T, Tachimiri ME, Klersy C, Ticozzelli G, Bellinzona G, Blangetti I, et al Near infrared spectroscopy monitoring during carotid endarterectomy: which threshold value is critical? Eur J Vasc Endovasc Surg 2004; 27: 646–650. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
