

Pathophysiology and Management of Acute Respiratory Distress Syndrome in Children
- PMID: 28941533
- PMCID: PMC9683071
- DOI: 10.1016/j.pcl.2017.06.004
Pathophysiology and Management of Acute Respiratory Distress Syndrome in Children
Abstract
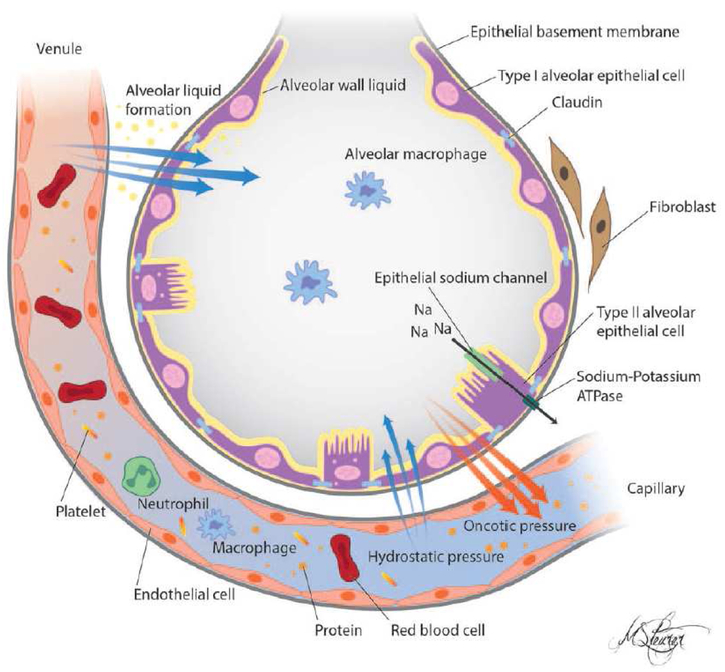
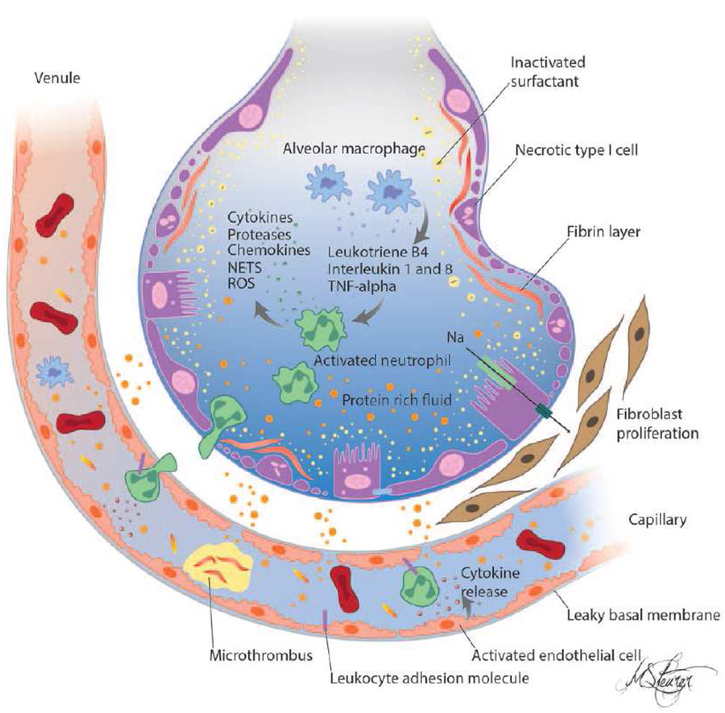
Acute respiratory distress syndrome (ARDS) is a syndrome of noncardiogenic pulmonary edema and hypoxia that accompanies up to 30% of deaths in pediatric intensive care units. Pediatric ARDS (PARDS) is diagnosed by the presence of hypoxia, defined by oxygenation index or Pao2/Fio2 ratio cutoffs, and new chest infiltrate occurring within 7 days of a known insult. Hallmarks of ARDS include hypoxemia and decreased lung compliance, increased work of breathing, and impaired gas exchange. Mortality is often accompanied by multiple organ failure. Although many modalities to treat PARDS have been investigated, supportive therapies and lung protective ventilator support remain the mainstay.
Keywords: Acute lung injury; Acute respiratory distress syndrome; PARDS; Pathophysiology; Pediatrics.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
