

Effects of Androgen Deprivation Therapy on Pain Perception, Quality of Life, and Depression in Men With Prostate Cancer
- PMID: 28941963
- PMCID: PMC5794536
- DOI: 10.1016/j.jpainsymman.2017.09.017
Effects of Androgen Deprivation Therapy on Pain Perception, Quality of Life, and Depression in Men With Prostate Cancer
Abstract
Context: Previous animal and human research suggests that testosterone has antinociceptive properties. Castration in male rodents increases pain perception which is reversed by testosterone replacement. Pain perception also improves in hypogonadal men with testosterone therapy. However, it remains unclear whether androgen deprivation therapy (ADT) in men with prostate cancer (PCa) is associated with an increase in pain perception.
Objectives: To evaluate the effects of ADT on pain perception, depression and quality of life (QOL) in men with PCa.
Methods: Thirty-seven men with PCa about to undergo ADT with leuprolide acetate (ADT group) were followed prospectively for six months to evaluate changes in clinical and experimental pain. Forty men who had previously undergone prostatectomy for localized PCa and were in remission served as controls (non-ADT group). All participants were eugonadal at study entry. Primary outcomes were changes in clinical pain (assessed with Brief Pain Inventory questionnaire) and experimental pain (assessed with quantitative sensory testing). Secondary outcomes included evaluation of depression, anxiety levels, and quality of life.
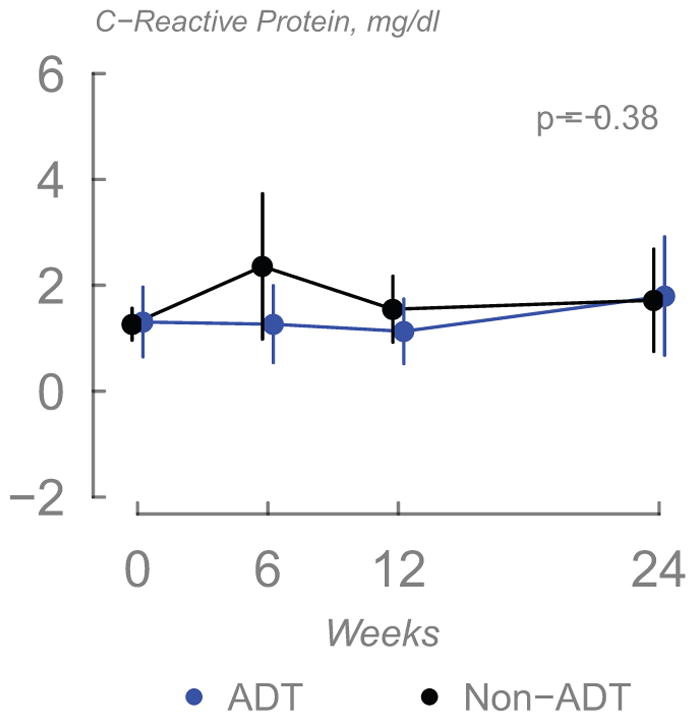
Results: Serum testosterone levels significantly decreased in the ADT group but remained unchanged in the non-ADT group. There were no significant changes in pain thresholds, ratings, or other responses to quantitative sensory tests over the 6-month course of the study. Clinical pain did not differ between the two groups, and no changes from baseline were observed in either group. Men undergoing ADT did experience worsening of depression (0.93; 95% CI = 0.04-1.82; P = 0.042) and QOL related to physical role limitation (-18.28; 95% CI = -30.18 to -6.37; P = 0.003).
Conclusion: ADT in men with PCa is associated with worsening of depression scores and QOL but is not associated with changes in clinical pain or pain sensitivity.
Keywords: GnRH agonists; Prostate cancer; depression; pain perception; pain tolerance; quality of life; quantitative sensory testing; testosterone.
Copyright © 2017 American Academy of Hospice and Palliative Medicine. Published by Elsevier Inc. All rights reserved.
Figures






Similar articles
-
Long-term effects of androgen deprivation therapy in prostate cancer patients.Clin Endocrinol (Oxf). 2002 Jun;56(6):779-86. doi: 10.1046/j.1365-2265.2002.01551.x. Clin Endocrinol (Oxf). 2002. PMID: 12072048
-
Depressive symptoms are found to be potential adverse effects of androgen deprivation therapy in older prostate cancer patients: A 15-month prospective, observational study.Psychooncology. 2017 Dec;26(12):2238-2244. doi: 10.1002/pon.4453. Epub 2017 May 31. Psychooncology. 2017. PMID: 28474429
-
Metabolic Changes in Androgen-Deprived Nondiabetic Men With Prostate Cancer Are Not Mediated by Cytokines or aP2.J Clin Endocrinol Metab. 2018 Oct 1;103(10):3900-3908. doi: 10.1210/jc.2018-01068. J Clin Endocrinol Metab. 2018. PMID: 30032274 Free PMC article. Clinical Trial.
-
The effect of androgen deprivation therapy on health-related quality of life in men with prostate cancer.Urology. 2001 Aug;58(2 Suppl 1):94-100. doi: 10.1016/s0090-4295(01)01250-x. Urology. 2001. PMID: 11502459 Review.
-
Contemporary role of androgen deprivation therapy for prostate cancer.Eur Urol. 2012 Jan;61(1):11-25. doi: 10.1016/j.eururo.2011.08.026. Epub 2011 Aug 19. Eur Urol. 2012. PMID: 21871711 Free PMC article. Review.
Cited by
-
Pain sensitivity and quality of life of patients with burning mouth syndrome: a preliminary study in a Chinese population.BMC Oral Health. 2023 Dec 1;23(1):951. doi: 10.1186/s12903-023-03689-2. BMC Oral Health. 2023. PMID: 38041054 Free PMC article.
-
Mechanisms responsible for reduced erythropoiesis during androgen deprivation therapy in men with prostate cancer.Am J Physiol Endocrinol Metab. 2018 Dec 1;315(6):E1185-E1193. doi: 10.1152/ajpendo.00272.2018. Epub 2018 Oct 16. Am J Physiol Endocrinol Metab. 2018. PMID: 30325657 Free PMC article.
-
Changes in Quality of Life and Sexual Function After Luteinizing Hormone-Releasing Hormone (LHRH) Agonists and Orchiectomy in Men With Metastatic Prostate Cancer: Results From a Randomized Trial.Cureus. 2024 Mar 11;16(3):e55934. doi: 10.7759/cureus.55934. eCollection 2024 Mar. Cureus. 2024. PMID: 38601370 Free PMC article.
-
Hypothalamic connectivities predict individual differences in ADT-elicited changes in working memory and quality of life in prostate cancer patients.Sci Rep. 2022 Jun 10;12(1):9567. doi: 10.1038/s41598-022-13361-4. Sci Rep. 2022. PMID: 35688928 Free PMC article.
-
Androgen Deprivation Therapy for Prostate Cancer: Focus on Cognitive Function and Mood.Medicina (Kaunas). 2023 Dec 30;60(1):77. doi: 10.3390/medicina60010077. Medicina (Kaunas). 2023. PMID: 38256338 Free PMC article. Review.
References
-
- Unruh AM. Gender variations in clinical pain experience. Pain. 1996;65:123–167. - PubMed
-
- Sternbach RA. Pain and ‘hassles’ in the United States: findings of the Nuprin pain report. Pain. 1986;27:69–80. - PubMed
-
- Aloisi AM, Ceccarelli I, Fiorenzani P. Gonadectomy affects hormonal and behavioral responses to repetitive nociceptive stimulation in male rats. Ann N Y Acad Sci. 2003;1007:232–237. - PubMed
-
- Melchior M, Poisbeau P, Gaumond I, Marchand S. Insights into the mechanisms and the emergence of sex-differences in pain. Neuroscience. 2016;338:63–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
