

Impact of acute left ventricular apical thrombus on cardioversion for atrial fibrillation
- PMID: 28942610
- PMCID: PMC6351065
- DOI: 10.1111/echo.13706
Impact of acute left ventricular apical thrombus on cardioversion for atrial fibrillation
Abstract
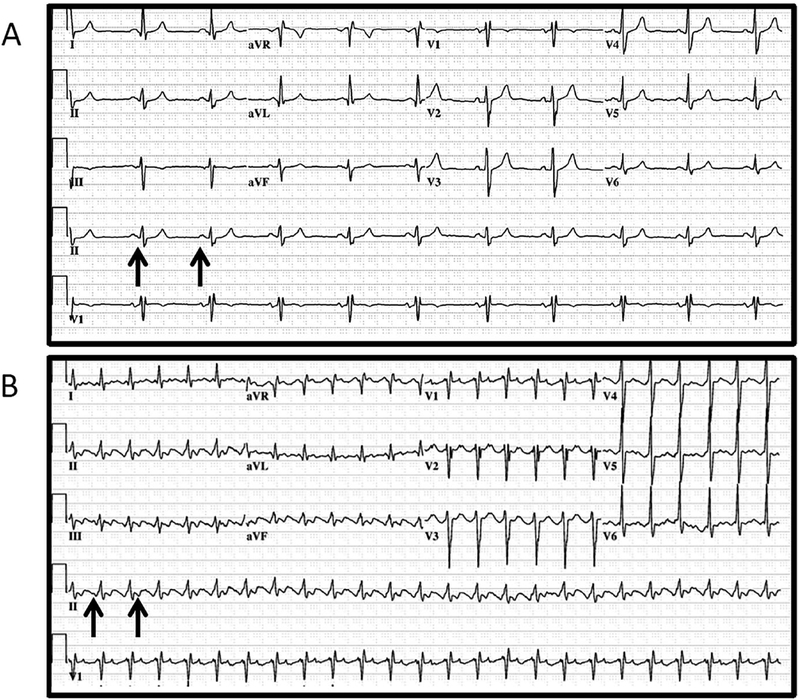
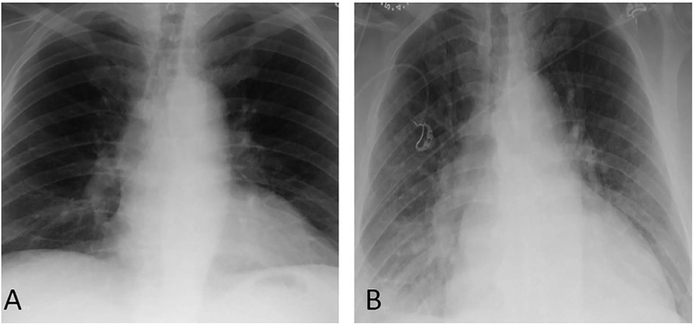
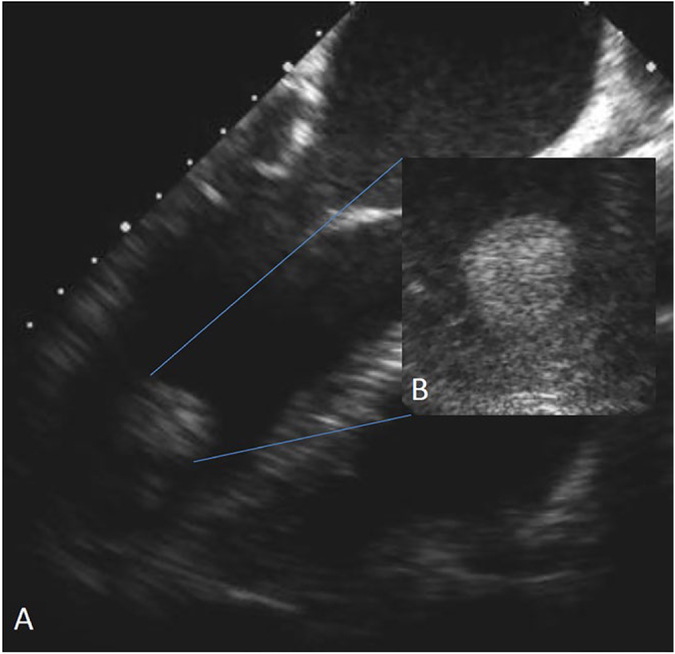
Among patients undergoing cardioversion for atrial fibrillation, the presence of left ventricular thrombus is a relatively uncommon and challenging clinical dilemma. While left atrial appendage thrombus is a contraindication to cardioversion, there is paucity of data regarding the safety of cardioversion in with the presence of left ventricular apical thrombus. Also, thrombus characteristics such as protrusion and mobility on echocardiography are known risk factors for systemic embolism. In this article, we present a case highlighting the management of atrial fibrillation in the setting of left ventricular dysfunction, acute heart failure, and echocardiographic evidence of acute left ventricular apical thrombus.
Keywords: atrial fibrillation; cardioversion; embolism; thrombus.
© 2017, Wiley Periodicals, Inc.
Figures
Similar articles
-
Transesophageal echocardiography before and during direct current cardioversion of atrial fibrillation: evidence for "atrial stunning" as a mechanism of thromboembolic complications.J Am Coll Cardiol. 1994 Feb;23(2):307-16. doi: 10.1016/0735-1097(94)90412-x. J Am Coll Cardiol. 1994. PMID: 8294679
-
Left atrial appendage thrombus is not uncommon in patients with acute atrial fibrillation and a recent embolic event: a transesophageal echocardiographic study.J Am Coll Cardiol. 1995 Feb;25(2):452-9. doi: 10.1016/0735-1097(94)00396-8. J Am Coll Cardiol. 1995. PMID: 7829800
-
Should all patients undergo transesophageal echocardiography before electrical cardioversion of atrial fibrillation?J Am Coll Cardiol. 1994 Feb;23(2):533-41. doi: 10.1016/0735-1097(94)90443-x. J Am Coll Cardiol. 1994. PMID: 8294710 Review.
-
A Suspected Case of Acute Embolic Myocardial Infarction Following Direct-Current Cardioversion of Atrial Fibrillation.Am J Case Rep. 2018 Nov 2;19:1306-1310. doi: 10.12659/AJCR.911469. Am J Case Rep. 2018. PMID: 30385736 Free PMC article. Review.
-
Exclusion of atrial thrombus by transesophageal echocardiography does not preclude embolism after cardioversion of atrial fibrillation.Circulation. 1994 Dec;90(6):3122. Circulation. 1994. PMID: 7994866 No abstract available.
Cited by
-
Management of left ventricular thrombus: a narrative review.Ann Transl Med. 2021 Mar;9(6):520. doi: 10.21037/atm-20-7839. Ann Transl Med. 2021. PMID: 33850917 Free PMC article. Review.
-
Atrial fibrillation-induced cardiomyopathy presenting with bilateral intermittent claudication associated with intracardiac thrombi.BMJ Case Rep. 2024 Mar 6;17(3):e257151. doi: 10.1136/bcr-2023-257151. BMJ Case Rep. 2024. PMID: 38453224
References
-
- January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:e199–267. - PMC - PubMed
-
- Vaitkus PT, Barnathan ES. Embolic potential, prevention and management of mural thrombus complicating anterior myocardial infarction: a meta-analysis. J Am Coll Cardiol. 1993;22:1004–1009. - PubMed
-
- Keren A, Goldberg S, Gottlieb S, et al. Natural history of left ventricular thrombi: their appearance and resolution in the posthospitalization period of acute myocardial infarction. J Am Coll Cardiol. 1990;15:790–800. - PubMed
-
- Visser CA, Kan G, Meltzer RS, Dunning AJ, Roelandt J. Embolic potential of left ventricular thrombus after myocardial infarction: a two-dimensional echocardiographic study of 119 patients. J Am Coll Cardiol. 1985;5:1276–1280. - PubMed
-
- Stratton JR, Resnick AD. Increased embolic risk in patients with left ventricular thrombi. Circulation. 1987;75:1004–1011. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
