

Lobar Emphysema Distribution Is Associated With 5-Year Radiological Disease Progression
- PMID: 28943279
- PMCID: PMC6026264
- DOI: 10.1016/j.chest.2017.09.022
Lobar Emphysema Distribution Is Associated With 5-Year Radiological Disease Progression
Abstract
Background: Emphysema has considerable variability in its regional distribution. Craniocaudal emphysema distribution is an important predictor of the response to lung volume reduction. However, there is little consensus regarding how to define upper lobe-predominant and lower lobe-predominant emphysema subtypes. Consequently, the clinical and genetic associations with these subtypes are poorly characterized.
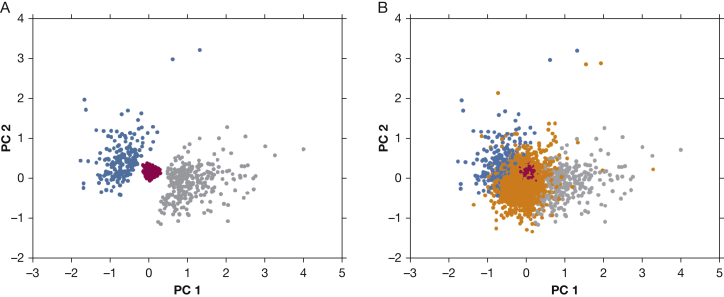
Methods: We sought to identify subgroups characterized by upper-lobe or lower-lobe emphysema predominance and comparable amounts of total emphysema by analyzing data from 9,210 smokers without alpha-1-antitrypsin deficiency in the Genetic Epidemiology of COPD (COPDGene) cohort. CT densitometric emphysema was measured in each lung lobe. Random forest clustering was applied to lobar emphysema variables after regressing out the effects of total emphysema. Clusters were tested for association with clinical and imaging outcomes at baseline and at 5-year follow-up. Their associations with genetic variants were also compared.
Results: Three clusters were identified: minimal emphysema (n = 1,312), upper lobe-predominant emphysema (n = 905), and lower lobe-predominant emphysema (n = 796). Despite a similar amount of total emphysema, the lower-lobe group had more severe airflow obstruction at baseline and higher rates of metabolic syndrome compared with subjects with upper-lobe predominance. The group with upper-lobe predominance had greater 5-year progression of emphysema, gas trapping, and dyspnea. Differential associations with known COPD genetic risk variants were noted.
Conclusions: Subgroups of smokers defined by upper-lobe or lower-lobe emphysema predominance exhibit different functional and radiological disease progression rates, and the upper-lobe predominant subtype shows evidence of association with known COPD genetic risk variants. These subgroups may be useful in the development of personalized treatments for COPD.
Trial registration: ClinicalTrials.gov NCT00608764.
Keywords: COPD; COPD disease progression; clustering; emphysema distribution; machine learning.
Copyright © 2017 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Han M.K., Bartholmai B., Liu L.X. Clinical significance of radiologic characterizations in COPD. COPD. 2009;6(6):459–467. - PubMed
-
- Venuta F., Anile M., Diso D. Long-term follow-up after bronchoscopic lung volume reduction in patients with emphysema. Eur Respir J. 2012;39(5):1084–1089. - PubMed
-
- Deslee G., Mal H., Dutau H. Lung volume reduction coil treatment vs usual care in patients with severe emphysema: The REVOLENS randomized clinical trial. JAMA. 2016;315(2):175–184. - PubMed
-
- Sciurba F.C., Chandra D., Bon J. Bronchoscopic lung volume reduction in COPD: lessons in implementing clinically based precision medicine. JAMA. 2016;315(2):139–141. - PubMed
-
- Fishman A., Martinez F., Naunheim K. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med. 2003;348(21):2059–2073. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- R01 HL113264/HL/NHLBI NIH HHS/United States
- R01 HL089897/HL/NHLBI NIH HHS/United States
- S10 OD018526/OD/NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- U01 HL089897/HL/NHLBI NIH HHS/United States
- R01 HL089856/HL/NHLBI NIH HHS/United States
- U01 HL089856/HL/NHLBI NIH HHS/United States
- K08 HL141601/HL/NHLBI NIH HHS/United States
- R01 HL126596/HL/NHLBI NIH HHS/United States
- K12 HL120004/HL/NHLBI NIH HHS/United States
- R01 HL124233/HL/NHLBI NIH HHS/United States
- P01 HL114501/HL/NHLBI NIH HHS/United States
- T32 HL007427/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
