

Endoscopic Ultrasound-guided Rendezvous Technique after Failed Endoscopic Retrograde Cholangiopancreatography: Which Approach Route Is the Best?
- PMID: 28943555
- PMCID: PMC5742383
- DOI: 10.2169/internalmedicine.8677-16
Endoscopic Ultrasound-guided Rendezvous Technique after Failed Endoscopic Retrograde Cholangiopancreatography: Which Approach Route Is the Best?
Abstract
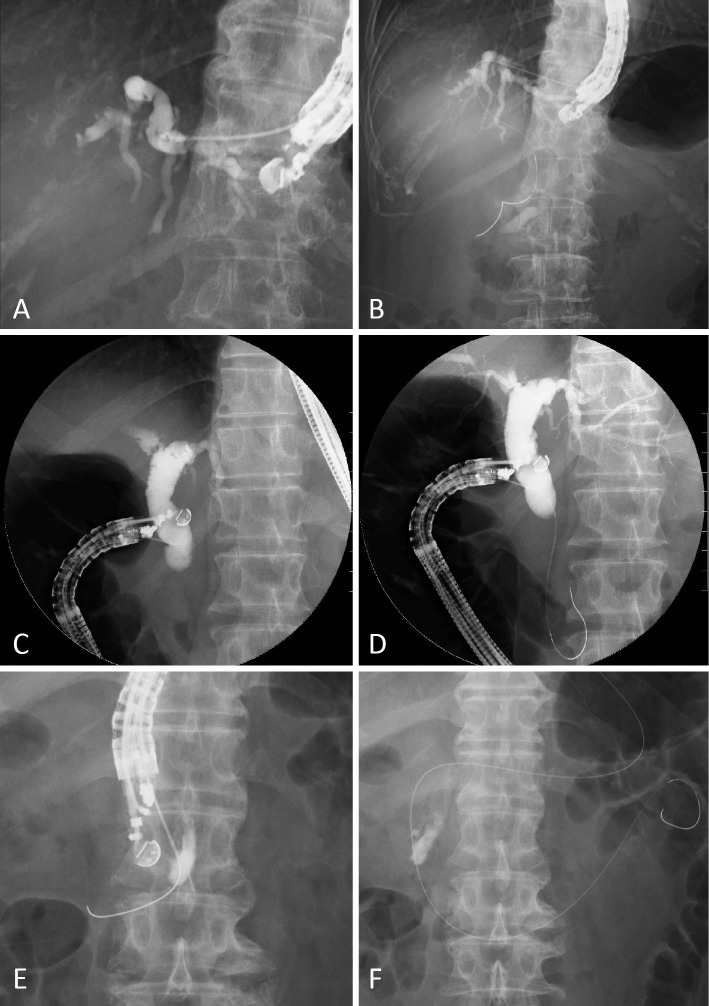
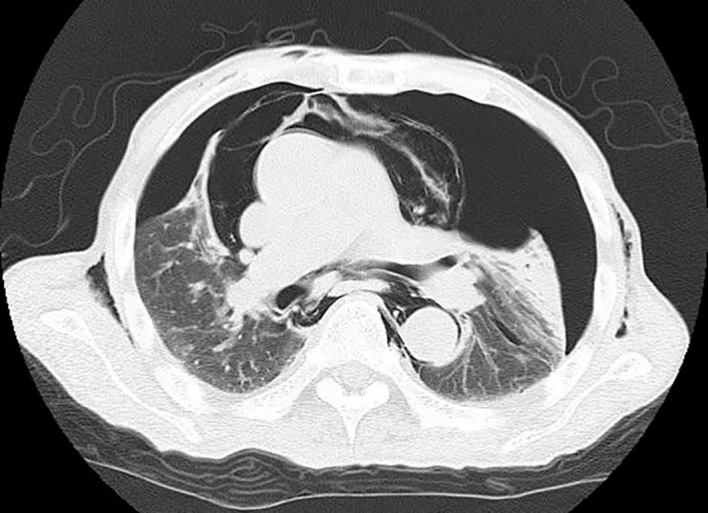
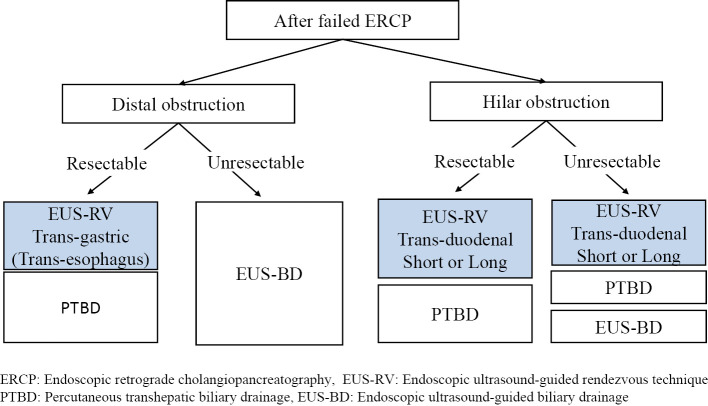
Objective The endoscopic ultrasound-guided rendezvous technique (EUS-RV) is a salvage method for failed selective biliary cannulation. Three puncture routes have been reported, with many comparisons between the intra-hepatic and extra-hepatic biliary ducts. We used the trans-esophagus (TE) and trans-jejunum (TJ) routes. In the present study, the utility of EUS-RV for biliary access was evaluated, focusing on the approach routes. Methods and Patients In 39 patients, 42 puncture routes were evaluated in detail. EUS-RV was performed between January 2010 and December 2014. The patients were prospectively enrolled, and their clinical data were retrospectively collected. Results The patients' median age was 71 (range 29-84) years. The indications for endoscopic retrograde cholangiopancreatography (ERCP) were malignant biliary obstruction in 24 patients and benign biliary disease in 15. The technical success rate was 78.6% (33/42) and was similar among approach routes (p=0.377). The overall complication rate was 16.7% (7/42) and was similar among approach routes (p=0.489). However, mediastinal emphysema occurred in 2 TE route EUS-RV patients. No EUS-RV-related deaths occurred. Conclusion EUS-RV proved reliable after failed ERCP. The selection of the appropriate route based on the patient's condition is crucial.
Keywords: ERCP; EUS; EUS-RV.
Figures

Similar articles
-
Endoscopic ultrasound-guided biliary rendezvous after failed cannulation, and comparison between benign vs malignant biliopancreatic disorders: outcomes at a single tertiary-care centre.Ann Med. 2024 Dec;56(1):2416607. doi: 10.1080/07853890.2024.2416607. Epub 2024 Oct 20. Ann Med. 2024. PMID: 39428568 Free PMC article.
-
Clinical utility of an endoscopic ultrasound-guided rendezvous technique via various approach routes.Surg Endosc. 2013 Sep;27(9):3437-43. doi: 10.1007/s00464-013-2896-5. Epub 2013 Mar 19. Surg Endosc. 2013. PMID: 23508814
-
Endoscopic Ultrasound-Guided Rendezvous Technique for Failed Biliary Cannulation in Benign and Resectable Malignant Biliary Disorders.Dig Dis Sci. 2018 Mar;63(3):787-796. doi: 10.1007/s10620-018-4908-8. Epub 2018 Jan 18. Dig Dis Sci. 2018. PMID: 29349694
-
Endoscopic ultrasound-guided rendezvous techniques for difficult biliary cannulation: Technical review.Dig Endosc. 2025 Jan;37(1):68-76. doi: 10.1111/den.14908. Epub 2024 Aug 28. Dig Endosc. 2025. PMID: 39193796 Review.
-
Endoscopic ultrasonography-guided biliary drainage: rendezvous technique.Gastrointest Endosc Clin N Am. 2012 Apr;22(2):249-58, viii-ix. doi: 10.1016/j.giec.2012.04.018. Epub 2012 May 9. Gastrointest Endosc Clin N Am. 2012. PMID: 22632947 Review.
Cited by
-
Therapeutic interventional endoscopic ultrasound in pancreato-biliary disorders: Does it really replace the surgical/percutaneous approach?World J Gastrointest Surg. 2021 Jun 27;13(6):537-547. doi: 10.4240/wjgs.v13.i6.537. World J Gastrointest Surg. 2021. PMID: 34194612 Free PMC article. Review.
-
A retrospective multicenter study comparing the punctures to B2 and B3 in endoscopic ultrasound-guided hepaticogastrostomy.DEN Open. 2023 Jan 3;3(1):e201. doi: 10.1002/deo2.201. eCollection 2023 Apr. DEN Open. 2023. PMID: 36618883 Free PMC article.
-
Endoscopic ultrasound-guided rendezvous technique in a transduodenal long endoscopic position using a 22 G needle combined with a novel 0.018-inch guidewire.Endoscopy. 2023 Dec;55(S 01):E379-E381. doi: 10.1055/a-1997-0460. Epub 2023 Jan 31. Endoscopy. 2023. PMID: 36720266 Free PMC article. No abstract available.
-
The Latest Advancements in Diagnostic Role of Endosonography of Pancreatic Lesions.J Clin Med. 2023 Jul 12;12(14):4630. doi: 10.3390/jcm12144630. J Clin Med. 2023. PMID: 37510744 Free PMC article. Review.
-
Controversies in Endoscopic Ultrasound-Guided Biliary Drainage.Cancers (Basel). 2024 Apr 23;16(9):1616. doi: 10.3390/cancers16091616. Cancers (Basel). 2024. PMID: 38730570 Free PMC article. Review.
References
-
- Sasahira N, Kawakami H, Isayama H, et al. . Early use of double-guide wire technique to facilitate selective bile duct cannulation: the multicenter randomized controlled EDUCATION trial. Endoscopy 47: 421-429, 2015. - PubMed
-
- Bailey AA, Bourke MJ, Williams SJ, et al. . A prospective randomized trial of cannulation technique in ERCP: effects on technical success and post-ERCP pancreatitis. Endoscopy 40: 296-301, 2008. - PubMed
-
- Kaffes AJ, Sriram PV, Rao GV, Santosh D, Reddy DN. Early institution of pre-cutting for difficult biliary cannulation: a prospective study comparing conventional vs. a modified technique. Gastrointest Endosc 62: 669-674, 2005. - PubMed
-
- Smith AC, Dowsett JF, Russell RC, Hatfield AR, Cotton PB. Randomised trial of endoscopic stenting versus surgical bypass in malignant low bileduct obstruction. Lancet 334: 1655-1660, 1994. - PubMed
-
- Kama NA, Coskun T, Yuksek YN, Yazgan A. Factors affecting post-operative mortality in malignant biliary tract obstruction. Hepatogastroenterology 46: 103-107, 1999. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources