

Hepatectomy for spontaneous rupture of hepatocellular carcinoma without portal triad clamping
- PMID: 28943906
- PMCID: PMC5592858
- DOI: 10.3892/ol.2017.6654
Hepatectomy for spontaneous rupture of hepatocellular carcinoma without portal triad clamping
Abstract
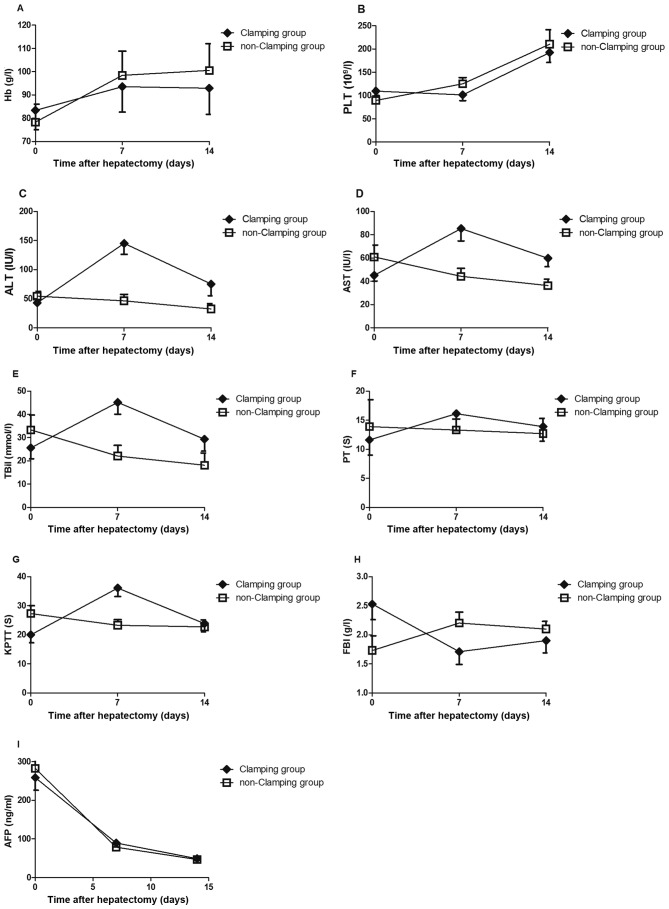
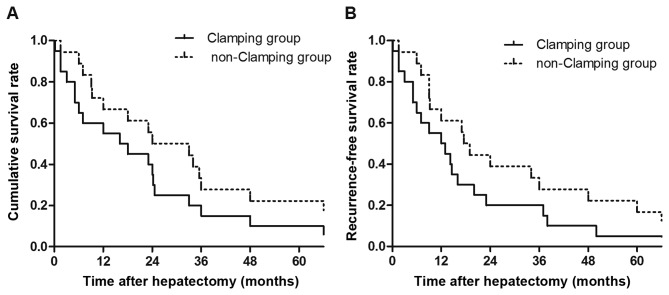
Hepatectomy without portal triad clamping may decrease the incidence of liver injury; however, the effects of hepatectomy without portal triad clamping in the treatment of spontaneous rupture of hepatocellular carcinoma (SRHCC) remain unclear. The aims of the present study were to evaluate the therapeutic value of hepatectomy without portal triad clamping in the treatment of patients with SRHCC. The present study retrospectively reviewed patients with SRHCC who received hepatectomy without portal triad clamping (non-clamping group) and the therapeutic efficacy was compared with that of 20 patients with SRHCC undergoing the same surgery in the presence of portal triad clamping (clamping group). Following hepatectomy, the non-clamping group exhibited a significantly lower incidence of acute liver failure compared with the clamping group (P<0.05). No significant differences in operative time, intra-operative blood loss, disease-free or overall survival times between the two groups were identified (all P>0.05). At 1 week and 2 weeks after surgery, the non-clamping group exhibited significantly lower alanine aminotransferase, aspartate aminotransferase and total bilirubin serum levels compared with the clamping group (all P<0.05). Hepatectomy without portal triad clamping may decrease the incidence of liver injury and liver failure in patients with SRHCC, suggesting that it may be a safe and effective therapeutic strategy.
Keywords: hepatectomy; portal triad clamping; spontaneous rupture.
Figures
Similar articles
-
Continuous versus intermittent portal triad clamping during hepatectomy in cirrhosis. Results of a prospective, randomized clinical trial.Hepatogastroenterology. 2003 Jul-Aug;50(52):1073-7. Hepatogastroenterology. 2003. PMID: 12845985 Clinical Trial.
-
Prolonged portal triad clamping during liver surgery for colorectal liver metastases is associated with decreased time to hepatic tumour recurrence.Eur J Surg Oncol. 2010 Feb;36(2):182-8. doi: 10.1016/j.ejso.2009.10.016. Epub 2009 Nov 18. Eur J Surg Oncol. 2010. PMID: 19926242
-
Selective main portal vein clamping to minimize the risk of recurrence after curative liver resection for hepatocellular carcinoma.Hepatogastroenterology. 2012 Jul-Aug;59(117):1560-5. doi: 10.5754/hge10174. Hepatogastroenterology. 2012. PMID: 22683973
-
Meta-analysis of Prognostic Factors for Overall Survival Among Resected Patients with Spontaneous Ruptured Hepatocellular Carcinoma.J Gastrointest Surg. 2023 Dec;27(12):2983-3000. doi: 10.1007/s11605-023-05860-0. Epub 2023 Nov 6. J Gastrointest Surg. 2023. PMID: 37932594 Review.
-
Spontaneously Ruptured Hepatocellular Carcinoma: Computed Tomography-Based Assessment.Diagnostics (Basel). 2023 Mar 7;13(6):1021. doi: 10.3390/diagnostics13061021. Diagnostics (Basel). 2023. PMID: 36980330 Free PMC article. Review.
Cited by
-
Retrospective analysis of transcatheter arterial chemoembolization treatment for spontaneously ruptured hepatocellular carcinoma.Oncol Lett. 2019 Dec;18(6):6423-6430. doi: 10.3892/ol.2019.11037. Epub 2019 Nov 1. Oncol Lett. 2019. PMID: 31807165 Free PMC article.
-
Transjugular intrahepatic portal shunt in the treatment of portal hypertension due to cirrhosis: single center experience.BMC Surg. 2019 Dec 12;19(1):191. doi: 10.1186/s12893-019-0659-5. BMC Surg. 2019. PMID: 31830972 Free PMC article.
-
Snip-electrocoagulation technique versus clamp-crashing technique for parenchyma transection in liver resection: a pilot study.Ann Transl Med. 2020 Jun;8(12):744. doi: 10.21037/atm-20-3019. Ann Transl Med. 2020. PMID: 32647669 Free PMC article.
References
-
- Kim PT, Su JC, Buczkowski AK, Schaeffer DF, Chung SW, Scudamore CH, Ho SG. Computed tomography and angiographic interventional features of ruptured hepatocellular carcinoma: Pictorial essay. Can Assoc Radiol J. 2006;57:159–168. - PubMed
-
- Lü XS, Zheng YS, Fan QQ. Liver resection for spontaneous rupture of primary hepatocellular carcinoma. The Chinese-German Journal of Clinical Oncology. 2003;2:23–24. doi: 10.1007/BF02835363. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources