

Clinical predictors of pathological complete response to neoadjuvant chemotherapy in triple-negative breast cancer
- PMID: 28943920
- PMCID: PMC5604131
- DOI: 10.3892/ol.2017.6692
Clinical predictors of pathological complete response to neoadjuvant chemotherapy in triple-negative breast cancer
Abstract
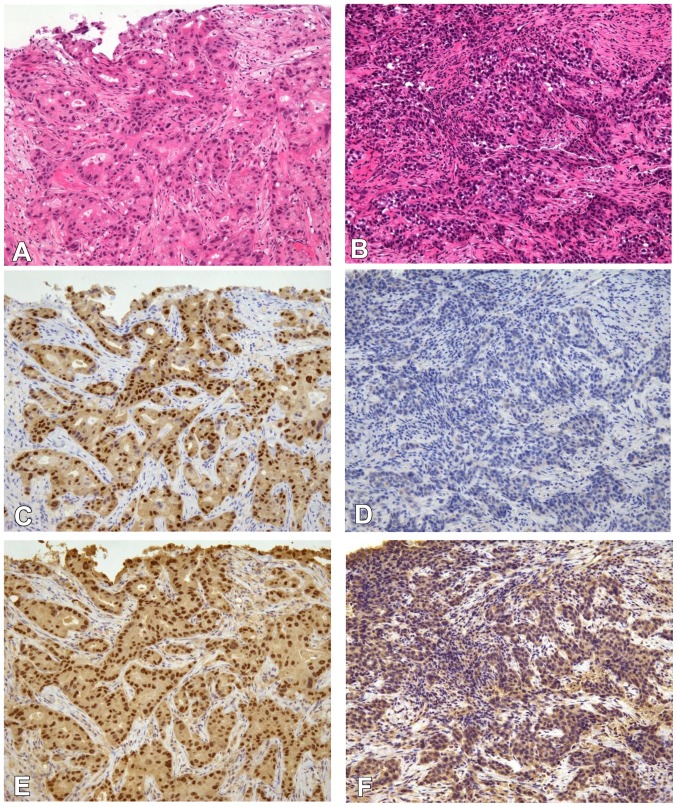
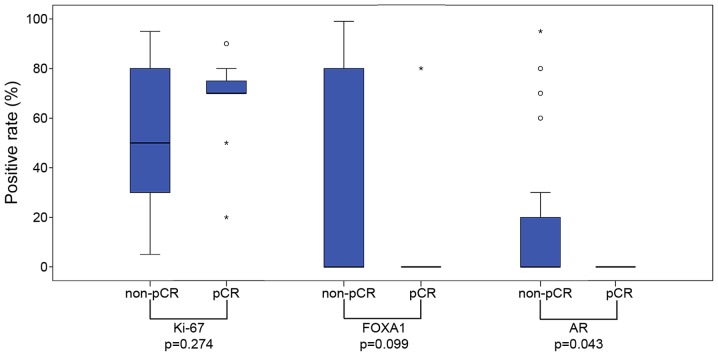
The response of triple-negative breast cancer (TNBC) to chemotherapy is heterogeneous; particular subtype classifications based on mRNA gene expression analysis have been demonstrated to be associated with a pathological complete response (pCR). The aim of the present study was to investigate additional clinical and pathological characteristics associated with pCR status. The pathological and clinical characteristics of 40 TNBC patients who underwent neoadjuvant chemotherapy followed by surgery were retrospectively analyzed by dividing the cases into two groups according to the response to treatment: pCR (n=12) and non-pCR (n=28). Clinically, patients in the pCR group presented tumors with a significantly less advanced Tumor-Node-Metastasis stage (P=0.030) and mammographic calcification was less common (17 vs. 58%; P=0.034). Pathologically, whereas all cases in the pCR group (12/12, 100%) were of the histological type 'invasive ductal carcinoma, not otherwise specified' (IDC-NOS), the non-pCR group consisted of a lower proportion of IDC-NOS cases (20/28, 71%) and more cases of special histological types, including mucinous, metaplastic, medullary and apocrine carcinomas (P=0.079). The positive rates of androgen receptor (AR) and forkhead-box A1 (FOXA1) tended to be lower in the pCR group (AR, 0 vs. 29%, P=0.079; FOXA1, 8 vs. 29%, P=0.233). The Ki-67 score was significantly higher in the pCR group than in the non-pCR group (P=0.041). The results suggest that patients with TNBC who present with clinically less advanced tumors and less frequent mammographic calcification are more likely to respond to chemotherapy. From a pathological standpoint, IDC-NOS type, negative AR status and higher Ki-67 scores may be associated with chemotherapy sensitivity.
Keywords: androgen receptor; mammographic calcifications; neoadjuvant chemotherapy; pathological complete response; triple-negative breast cancer.
Figures
Similar articles
-
The differences in the histological types of breast cancer and the response to neoadjuvant chemotherapy: the relationship between the outcome and the clinicopathological characteristics.Breast. 2012 Jun;21(3):289-95. doi: 10.1016/j.breast.2011.12.011. Epub 2012 Jan 25. Breast. 2012. PMID: 22277312
-
GATA-3 expression is not associated with complete pathological response in triple negative breast cancer patients treated with neoadjuvant chemotherapy.Pathol Res Pract. 2016 Jun;212(6):539-44. doi: 10.1016/j.prp.2016.03.004. Epub 2016 Mar 17. Pathol Res Pract. 2016. PMID: 27067807
-
Androgen receptor and FOXA1 coexpression define a "luminal-AR" subtype of feline mammary carcinomas, spontaneous models of breast cancer.BMC Cancer. 2019 Dec 30;19(1):1267. doi: 10.1186/s12885-019-6483-6. BMC Cancer. 2019. PMID: 31888566 Free PMC article.
-
Current strategy for triple-negative breast cancer: appropriate combination of surgery, radiation, and chemotherapy.Breast Cancer. 2011 Jul;18(3):165-73. doi: 10.1007/s12282-011-0254-9. Epub 2011 Feb 3. Breast Cancer. 2011. PMID: 21290263 Review.
-
Overview of resistance to systemic therapy in patients with breast cancer.Adv Exp Med Biol. 2007;608:1-22. doi: 10.1007/978-0-387-74039-3_1. Adv Exp Med Biol. 2007. PMID: 17993229 Review.
Cited by
-
Development and validation of a nomogram based on pretreatment dynamic contrast-enhanced MRI for the prediction of pathologic response after neoadjuvant chemotherapy for triple-negative breast cancer.Eur Radiol. 2022 Mar;32(3):1676-1687. doi: 10.1007/s00330-021-08291-0. Epub 2021 Nov 12. Eur Radiol. 2022. PMID: 34767068 Clinical Trial.
-
Pathological complete response to neoadjuvant chemotherapy in triple negative breast cancer - single hospital experience.Hered Cancer Clin Pract. 2023 Mar 16;21(1):4. doi: 10.1186/s13053-023-00249-1. Hered Cancer Clin Pract. 2023. PMID: 36922883 Free PMC article.
-
Clinical-pathologic characteristics and response to neoadjuvant chemotherapy in triple-negative low Ki-67 proliferation (TNLP) breast cancers.NPJ Breast Cancer. 2022 Apr 20;8(1):51. doi: 10.1038/s41523-022-00415-z. NPJ Breast Cancer. 2022. PMID: 35444182 Free PMC article.
-
Immune Landscape of Breast Cancers.Biomedicines. 2018 Feb 11;6(1):20. doi: 10.3390/biomedicines6010020. Biomedicines. 2018. PMID: 29439457 Free PMC article. Review.
-
Immunotyping of tumor-infiltrating lymphocytes in triple-negative breast cancer and genetic characterization.Oncol Lett. 2020 Nov;20(5):140. doi: 10.3892/ol.2020.12000. Epub 2020 Aug 20. Oncol Lett. 2020. PMID: 32934708 Free PMC article.
References
-
- Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: A population-based study from the California cancer registry. Cancer. 2007;109:1721–1728. doi: 10.1002/cncr.22618. - DOI - PubMed
-
- Lehmann BD, Jovanović B, Chen X, Estrada MV, Johnson KN, Shyr Y, Moses HL, Sanders ME, Pietenpol JA. Refinement of triple-negative breast cancer molecular subtypes: Implications for neoadjuvant chemotherapy selection. PLoS One. 2016;11:e0157368. doi: 10.1371/journal.pone.0157368. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials