

Comparison of Regional vs. General Anesthesia for Surgical Repair of Open-Globe Injuries at a University Referral Center
- PMID: 28944317
- PMCID: PMC5607023
- DOI: 10.1016/j.oret.2016.11.006
Comparison of Regional vs. General Anesthesia for Surgical Repair of Open-Globe Injuries at a University Referral Center
Abstract
Purpose: This study compares the clinical features and physician selection of either Regional Anesthesia (peribulbar or retrobulbar block) with Monitored Anesthesia Care (RA-MAC) or General Anesthesia (GA) for open globe injury repair.
Design: A non-randomized, comparative, retrospective case series at a University Referral Center.
Participants: All adult repairable open globe injuries receiving primary repair between January 1st, 2004 and December 31st, 2014 (11 years). Exclusion criteria were patients less than 18 years of age and those treated with primary enucleation.
Methods: Data was gathered via retrospective chart review.
Main outcome measures: Data collected from each patient was age, gender, injury type, location, length of wound, presenting visual acuity, classification of anesthesia used, duration of the procedure performed, months of clinical follow-up, and final visual acuity.
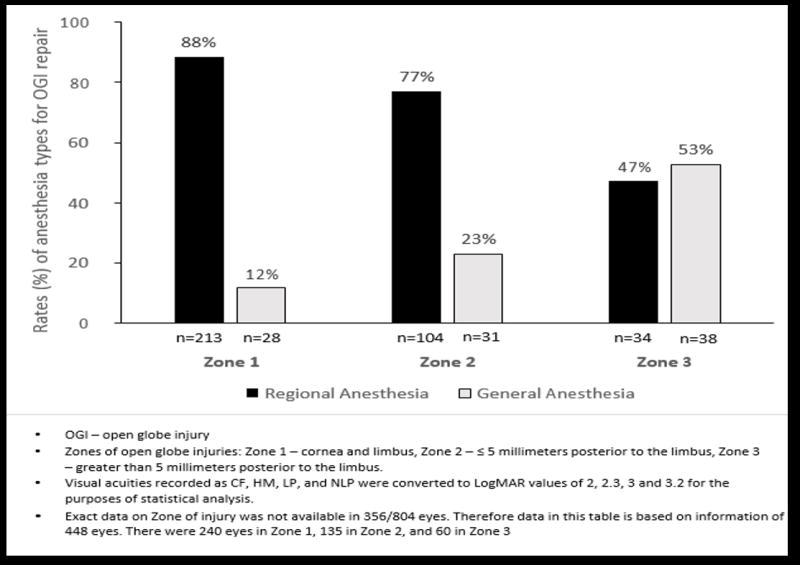
Results: During the 11 years study period, 448 patients were identified who had open globe injuries with documented information on zone of injury. Globe injury repair was performed using RA-MAC in 351/448 (78%) patients and general anesthesia in 97/448 (22%) patients. Zone 1, 2 and 3 injuries were recorded in 241, 135, and 72 patients respectively. The rates in specific zones, of RA-MAC versus GA were as follows: Zone 1 - 213/241 (88%) vs 28/241 (12%), Zone 2 - 104/135 (77%) vs 31/135 (23%) and Zone 3 - 34/72 (47%) vs 38/72 (53%). Open globe injuries repaired under RA-MAC had significantly shorter wound length (p<0.001), more anterior wound location (p<0.001) and shorter operative times (p<0.001). RA-MAC cases also had a better presenting and final visual acuity (p<0.001). Neither class of anesthesia conferred a greater visual acuity improvement (p=0.06). The use of GA did not cause any delay in the time elapsed from injury until surgical repair (p=0.74).
Conclusions: RA-MAC is a reasonable alternative to GA for the repair of open globe injuries in selected adult patients. RA-MAC was selected more often for Zone 1 and Zone 2 injuries. For eyes with Zone 3 injuries, there are equal selection ratio for RA-MAC and GA.
Conflict of interest statement
Conflict of Interest: No conflicting relationship exists for any author.
Figures
Similar articles
-
Evolving Use of Regional versus General Anesthesia for the Surgical Repair of Open Globe Injuries.Am J Ophthalmol. 2023 Jul;251:71-76. doi: 10.1016/j.ajo.2023.02.012. Epub 2023 Feb 22. Am J Ophthalmol. 2023. PMID: 36822572 Free PMC article. Clinical Trial.
-
Regional anesthesia with monitored anesthesia care for surgical repair of selected open globe injuries.Ophthalmic Surg Lasers Imaging. 2005 Mar-Apr;36(2):122-8. Ophthalmic Surg Lasers Imaging. 2005. PMID: 15792313
-
Local anesthesia with intravenous sedation for surgical repair of selected open globe injuries.Am J Ophthalmol. 2002 Nov;134(5):707-11. doi: 10.1016/s0002-9394(02)01692-6. Am J Ophthalmol. 2002. PMID: 12429247
-
Nail gun-induced open-globe injuries: a 10-year retrospective review.Retina. 2014 Feb;34(2):254-61. doi: 10.1097/IAE.0b013e3182979e0b. Retina. 2014. PMID: 23851631 Review.
-
Terror-related open-globe injuries: a 10-year review.Am J Ophthalmol. 2005 May;139(5):937-9. doi: 10.1016/j.ajo.2004.11.009. Am J Ophthalmol. 2005. PMID: 15860315 Review.
Cited by
-
Guideline for the treatment of no light perception eyes induced by mechanical ocular trauma.J Evid Based Med. 2022 Sep;15(3):302-314. doi: 10.1111/jebm.12496. Epub 2022 Sep 23. J Evid Based Med. 2022. PMID: 36151612 Free PMC article.
-
Evolving Use of Regional versus General Anesthesia for the Surgical Repair of Open Globe Injuries.Am J Ophthalmol. 2023 Jul;251:71-76. doi: 10.1016/j.ajo.2023.02.012. Epub 2023 Feb 22. Am J Ophthalmol. 2023. PMID: 36822572 Free PMC article. Clinical Trial.
-
Open Globe Injuries: Review of Evaluation, Management, and Surgical Pearls.Clin Ophthalmol. 2022 Aug 10;16:2545-2559. doi: 10.2147/OPTH.S372011. eCollection 2022. Clin Ophthalmol. 2022. PMID: 35983163 Free PMC article. Review.
References
-
- Meyer D, Hamilton RC, Loken RG, Gimbel HV. Effect of combined peribulbar and retrobulbar injection of large volumes of anesthetic agents on the intraocular pressure. Canadian journal of ophthalmology. Journal canadien d’ophtalmologie. 1992;27(5):230–232. - PubMed
-
- Parke DW, 3rd, Flynn HW, Jr, Fisher YL. Management of intraocular foreign bodies: a clinical flight plan. Canadian journal of ophthalmology. Journal canadien d’ophtalmologie. 2013;48(1):8–12. - PubMed
-
- Lincoff HA, Breinin GM, De Voe AG. The effect of succinylcholine on the extraocular muscles. Am J Ophthalmol. 1957;43(3):440–444. - PubMed
-
- Kelly RE, Dinner M, Turner LS, Haik B, Abramson DH, Daines P. Succinylcholine increases intraocular pressure in the human eye with the extraocular muscles detached. Anesthesiology. 1993;79(5):948–952. - PubMed
-
- Igboko JO, Desalu I, Akinsola FB, Kushimo OT. Intraocular pressure changes in a Nigerian population--effects of tracheal tube and laryngeal mask airway insertion and removal. Niger Postgrad Med J. 2009;16(2):99–104. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources