

Evaluation of the Alvarado scoring system in the management of acute appendicitis
- PMID: 28944334
- PMCID: PMC5602313
- DOI: 10.5152/turkjsurg.2017.3539
Evaluation of the Alvarado scoring system in the management of acute appendicitis
Abstract
Objective: In this study, we aimed to show the effectiveness of Alvarado score and its components to predict the correct diagnosis of acute appendicitis and to find an optimum cut-off value for Alvarado score.
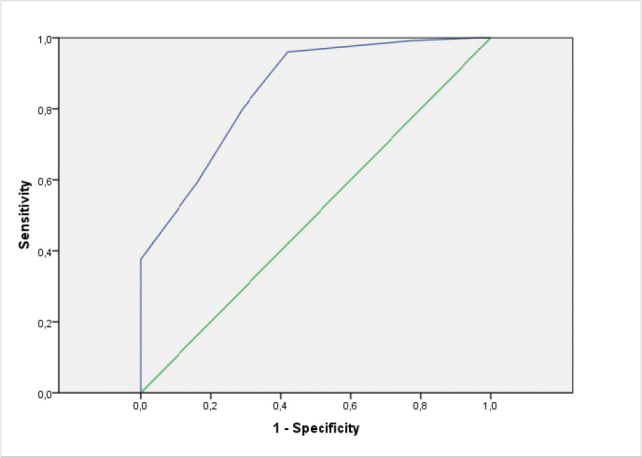
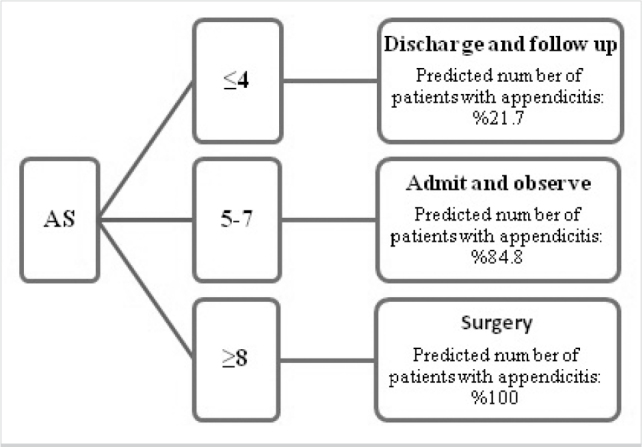
Material and methods: The patients who underwent surgical operation between January 2011 and January 2012 with the suspicion of acute appendicitis were included in the study. Their demographic and clinical features and histopathological results were retrieved from the medical records. They were divided into three groups according to their Alvarado scores. With the use of "receiver operating characteristic" curve analysis, the optimum cut-off value needed to make a correct diagnosis of acute appendicitis was determined.
Results: In all, 156 patients were included into the study. The mean age was 31.41±13.27 years. Histopathologically, acute appendicitis was detected in 125 (80.1%) patients, and negative appendectomy was found in 31 patients (19.8%). Mean Alvarado score was 6.44±1.49. There was a significant correlation between negative appendectomy and low Alvarado score (p<0.001). The main component of Alvarado score that makes the difference was rebound. Fever higher than 37.3°C, rebound, loss of appetite, and existence of shifting pain were statistically differential components (p=0.042, p<0.001, p=0.045, p<0.001, respectively). The rate of correct diagnosis of acute appendicitis was maximum in group 3 (100%) and minimum in group 1 (21.7%). Optimum cut-off value for Alvarado score was 7.
Conclusion: Patients with an Alvarado score of over 7 can be taken into surgical operation without the need of imaging methods.
Keywords: Acute appendicitis; Alvarado Score; cut-off value.
Conflict of interest statement
Conflict of Interest: No conflict of interest was declared by the authors.
Figures
Comment in
-
Editorial comment on: 'Evaluation of the Alvarado scoring system in the management of acute appendicitis'.Turk J Surg. 2017 Dec 1;33(4):320-321. doi: 10.5152/turkjsurg.2017.4002. eCollection 2017. Turk J Surg. 2017. PMID: 29260147 Free PMC article. No abstract available.
Similar articles
-
The comparison of the effectiveness of tomography and Alvarado scoring system in patients who underwent surgery with the diagnosis of appendicitis.Ulus Cerrahi Derg. 2015 Jun 24;32(2):111-4. doi: 10.5152/UCD.2015.2813. eCollection 2016. Ulus Cerrahi Derg. 2015. PMID: 27436935 Free PMC article.
-
Comparison of Raja Isteri Pengiran Anak Saleha Appendicitis and modified Alvarado scoring systems in the diagnosis of acute appendicitis.ANZ J Surg. 2020 Apr;90(4):521-524. doi: 10.1111/ans.15607. Epub 2019 Dec 15. ANZ J Surg. 2020. PMID: 31840385
-
Evaluation of modified Alvarado scoring system and RIPASA scoring system as diagnostic tools of acute appendicitis.World J Emerg Med. 2017;8(4):276-280. doi: 10.5847/wjem.j.1920-8642.2017.04.005. World J Emerg Med. 2017. PMID: 29123605 Free PMC article.
-
Diagnostic scores for acute appendicitis. Abdominal Pain Study Group.Eur J Surg. 1995 Apr;161(4):273-81. Eur J Surg. 1995. PMID: 7612771 Review.
-
Comparison of RIPASA and ALVARADO scores for risk assessment of acute appendicitis: A systematic review and meta-analysis.PLoS One. 2022 Sep 30;17(9):e0275427. doi: 10.1371/journal.pone.0275427. eCollection 2022. PLoS One. 2022. PMID: 36178953 Free PMC article.
Cited by
-
Editorial comment on: 'Evaluation of the Alvarado scoring system in the management of acute appendicitis'.Turk J Surg. 2017 Dec 1;33(4):320-321. doi: 10.5152/turkjsurg.2017.4002. eCollection 2017. Turk J Surg. 2017. PMID: 29260147 Free PMC article. No abstract available.
-
Nationwide prospective audit for the evaluation of appendicitis risk prediction models in adults: right iliac fossa treatment (RIFT)-Turkey.BJS Open. 2024 Sep 3;8(5):zrae120. doi: 10.1093/bjsopen/zrae120. BJS Open. 2024. PMID: 39383358 Free PMC article.
-
Accuracy of neutrophil lymphocyte ratio for diagnosis of acute appendicitis in children: A diagnostic study.Ann Med Surg (Lond). 2019 Oct 17;48:35-38. doi: 10.1016/j.amsu.2019.10.013. eCollection 2019 Dec. Ann Med Surg (Lond). 2019. PMID: 31687137 Free PMC article.
-
A rare presentation of an ectopic kidney with pyelonephritis mimicking appendicitis.J Surg Case Rep. 2019 Nov 20;2019(11):rjz342. doi: 10.1093/jscr/rjz342. eCollection 2019 Nov. J Surg Case Rep. 2019. PMID: 31768250 Free PMC article.
-
Diagnostic accuracy of Alvarado scoring system relative to histopathological diagnosis for acute appendicitis: A retrospective cohort study.Ann Med Surg (Lond). 2022 Sep 2;81:104561. doi: 10.1016/j.amsu.2022.104561. eCollection 2022 Sep. Ann Med Surg (Lond). 2022. PMID: 36147117 Free PMC article.
References
-
- Ohle R, O’Reilly F, O’Brien KK, Fahey T, Dimitrov BD. The Alvarado score for predicting acute appendicitis: a systematic review. BMC Med. 2011;9:139. https://doi.org/10.1186/1741-7015-9-139. - DOI - PMC - PubMed
-
- Al-Hashemy A, Seleem M. Appraisal of the modified Alvarado score for acute appendicitis in the adult. Saudi Med J. 2004;25:1229–1231. - PubMed
-
- Yildirim E, Karagülle E, Kirbaş I, Türk E, Hasdoğan B, Tekşam M, et al. Alvarado scores and pain onset in relation to multislice CT findings in acute appendicitis. Diagn Interv Radiol. 2008;14:14–18. - PubMed
-
- Park JS, Jeong JH, Lee JI, Lee JH, Park JK, Moon HJ. Accuracies of diagnostic methods for acute appendicitis. Am Surg. 2013;79:101–106. - PubMed
-
- Andersson RE. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br J Surg. 2004;91:28–37. https://doi.org/10.1002/bjs.4464. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources