

Radiogenomics of neuroblastomas: Relationships between imaging phenotypes, tumor genomic profile and survival
- PMID: 28945781
- PMCID: PMC5612658
- DOI: 10.1371/journal.pone.0185190
Radiogenomics of neuroblastomas: Relationships between imaging phenotypes, tumor genomic profile and survival
Abstract
Purpose: This study investigated relationships between neuroblastomas (NBs) imaging phenotypes, tumor genomic profile and patient outcome.
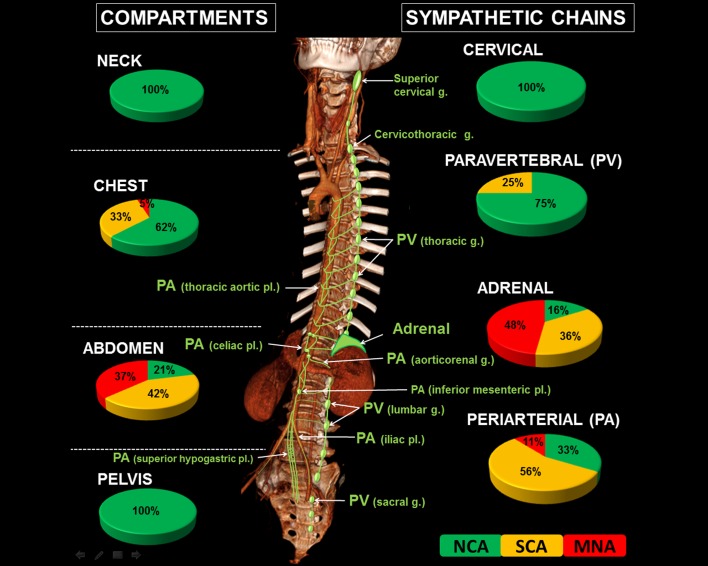
Patients and methods: This IRB-approved retrospective observational study included 133 NB patients (73 M, 60 F; median age 15 months, range 0-151) treated in a single institution between 1998 and 2012. A consensus review of imaging (CT-scan, MRI) categorized tumors according to both the primarily involved compartment (i.e., neck, chest, abdomen or pelvis) and the sympathetic anatomical structure the tumors rose from (i.e., cervical, paravertebral or periarterial chains, or adrenal gland). Tumor shape, volume and image-defined surgical risk factors (IDRFs) at diagnosis were recorded. Genomic profiles were assessed using array-based comparative genomic hybridization and divided into three groups: "numerical-only chromosome alterations" (NCA), "segmental chromosome alterations" (SCA) and "MYCN amplification" (MNA). Statistical analyses included Kruskal-Wallis, Chi2 and Fisher's exact tests and the Kaplan-Meier method with log-rank tests and Cox model for univariate and multivariate survival analyses.
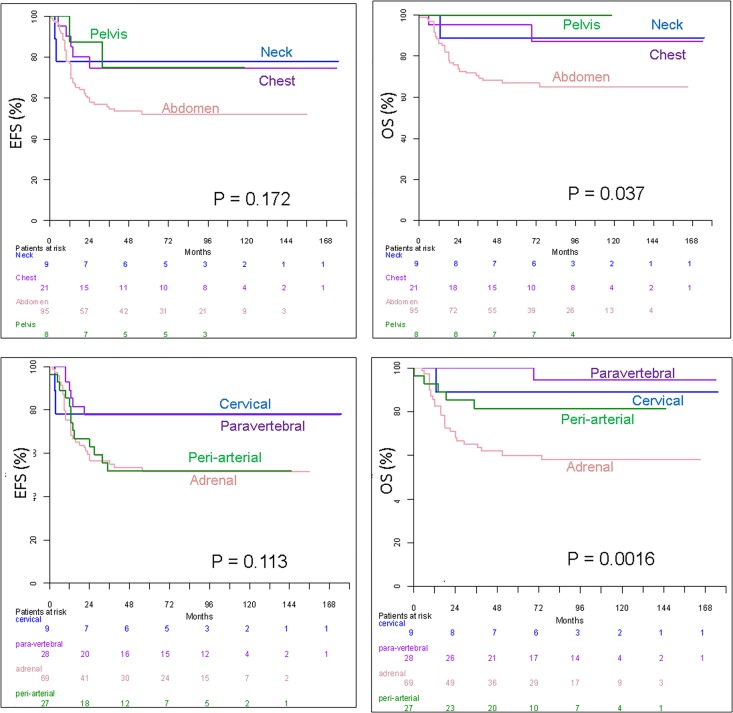
Results: A significant association between the sympathetic structure origin of tumors and genomic profiles was demonstrated. NBs arising from cervical sympathetic chains were all NCA. Paravertebral NBs were NCA or SCA in 75% and 25%, respectively and none were MNA. Periarterial NBs were NCA, SCA or MNA in 33%, 56% and 11%, respectively. Adrenal NBs were NCA, SCA or MNA in 16%, 36% and 48%, respectively. Among MNA NBs, 92% originated from the adrenal gland. The sympathetic anatomical classification was significantly better correlated to overall survival than the compartmental classification (P < .0003). The tumor volume of MNA NBs was significantly higher than NCA or SCA NBs (P < .0001). Patients with initial volume less than 160 mL had significantly better overall survival (P < .009). A "single mass" pattern was significantly more frequent in NCA NBs (P = .0003). The number of IDRFs was significantly higher in MNA NBs (P < .0001).
Conclusion: Imaging phenotypes of neuroblastomas, including tumor origin along the sympathetic system, correlate with tumor genomic profile and patient outcome.
Conflict of interest statement
Figures

Similar articles
-
Genomic Copy Number Profiling Using Circulating Free Tumor DNA Highlights Heterogeneity in Neuroblastoma.Clin Cancer Res. 2016 Nov 15;22(22):5564-5573. doi: 10.1158/1078-0432.CCR-16-0500. Epub 2016 Jul 20. Clin Cancer Res. 2016. PMID: 27440268
-
Loss of whole chromosome X predicts prognosis of neuroblastoma patients with numerical genomic profile.Pediatr Blood Cancer. 2019 May;66(5):e27635. doi: 10.1002/pbc.27635. Epub 2019 Jan 28. Pediatr Blood Cancer. 2019. PMID: 30688024
-
Correlation between the number of segmental chromosome aberrations and the age at diagnosis of diploid neuroblastomas without MYCN amplification.J Pediatr Surg. 2011 Dec;46(12):2228-32. doi: 10.1016/j.jpedsurg.2011.09.005. J Pediatr Surg. 2011. PMID: 22152855
-
Neuroblastoma.Urol Clin North Am. 2000 Aug;27(3):383-92, vii. doi: 10.1016/s0094-0143(05)70087-2. Urol Clin North Am. 2000. PMID: 10985139 Review.
-
How well do image-defined risk factors (IDRFs) predict surgical outcomes and survival in patients with neuroblastoma? A systematic review and meta-analysis.Pediatr Surg Int. 2020 Aug;36(8):897-907. doi: 10.1007/s00383-020-04696-y. Epub 2020 Jun 12. Pediatr Surg Int. 2020. PMID: 32533235
Cited by
-
Advancing therapy for neuroblastoma.Nat Rev Clin Oncol. 2022 Aug;19(8):515-533. doi: 10.1038/s41571-022-00643-z. Epub 2022 May 25. Nat Rev Clin Oncol. 2022. PMID: 35614230 Review.
-
[Imaging of abdominal tumors in childhood and adolescence : Part II: relevant intra-abdominal and retroperitoneal tumor entities].Radiologe. 2018 Jul;58(7):673-686. doi: 10.1007/s00117-018-0410-8. Radiologe. 2018. PMID: 29947934 German.
-
Stratification of Anatomical Imaging Features Between High-Risk and Non-High-Risk Groups in Neuroblastoma.Cancer Control. 2025 Jan-Dec;32:10732748251315883. doi: 10.1177/10732748251315883. Cancer Control. 2025. PMID: 39833998 Free PMC article.
-
CT-Based Radiomics Signature With Machine Learning Predicts MYCN Amplification in Pediatric Abdominal Neuroblastoma.Front Oncol. 2021 May 24;11:687884. doi: 10.3389/fonc.2021.687884. eCollection 2021. Front Oncol. 2021. PMID: 34109133 Free PMC article.
-
A subset of image-defined risk factors predict completeness of resection in children with high-risk neuroblastoma: An international multicenter study.Pediatr Blood Cancer. 2024 Oct;71(10):e31218. doi: 10.1002/pbc.31218. Epub 2024 Jul 28. Pediatr Blood Cancer. 2024. PMID: 39072986
References
-
- Takahashi Y, Sipp D, Enomoto H. Tissue interactions in neural crest cell development and disease. Science. 2013;341(6148):860–3. doi: 10.1126/science.1230717 . - DOI - PubMed
-
- Cohn SL, Pearson AD, London WB, Monclair T, Ambros PF, Brodeur GM, et al. The International Neuroblastoma Risk Group (INRG) classification system: an INRG Task Force report. J Clin Oncol. 2009;27(2):289–97. doi: 10.1200/JCO.2008.16.6785 ; PubMed Central PMCID: PMCPMC2650388. - DOI - PMC - PubMed
-
- Brodeur GM, Pritchard J, Berthold F, Carlsen NL, Castel V, Castelberry RP, et al. Revisions of the international criteria for neuroblastoma diagnosis, staging, and response to treatment. J Clin Oncol. 1993;11(8):1466–77. doi: 10.1200/JCO.1993.11.8.1466 . - DOI - PubMed
-
- Monclair T, Brodeur GM, Ambros PF, Brisse HJ, Cecchetto G, Holmes K, et al. The International Neuroblastoma Risk Group (INRG) staging system: an INRG Task Force report. J Clin Oncol. 2009;27(2):298–303. doi: 10.1200/JCO.2008.16.6876 ; PubMed Central PMCID: PMCPMC2650389. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
