

Management of traumatic urethral injuries in children using different techniques: A case series and review of literature
- PMID: 28946028
- PMCID: PMC5614720
- DOI: 10.1016/j.ijscr.2017.08.062
Management of traumatic urethral injuries in children using different techniques: A case series and review of literature
Abstract
Introduction: Most pediatric urethral injuries are a result of pelvic fracture after high-impact blunt trauma, mainly due to motor vehicle accidents. The management of urethral injuries depends on if the rupture is complete or partial as well as the timing of surgical intervention.
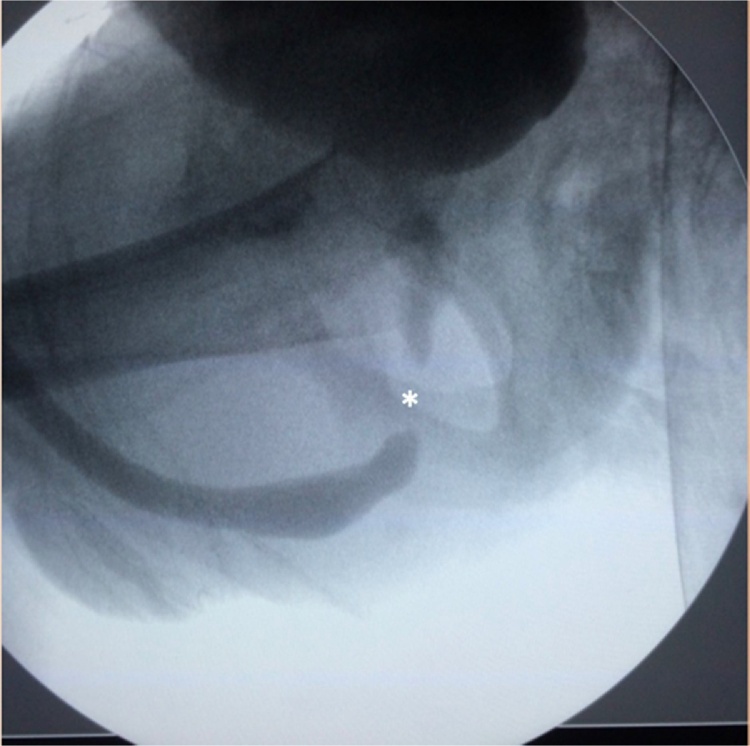
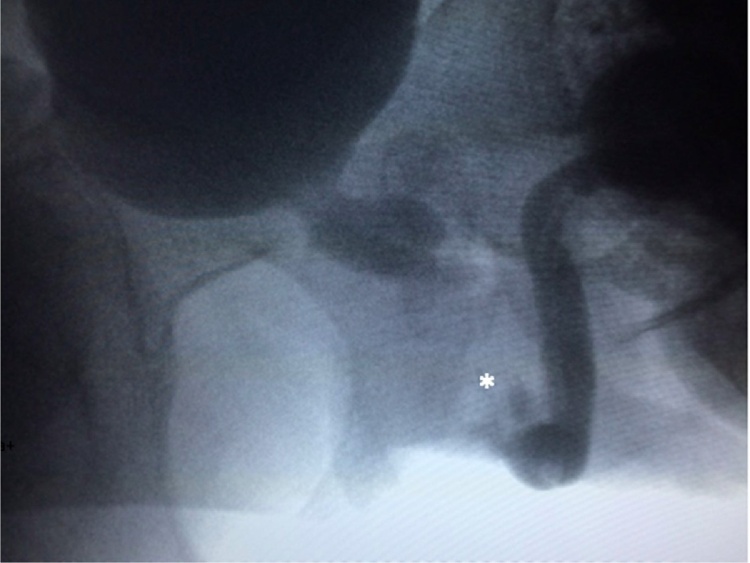
Presentation of cases: Three male children with urethral trauma caused by motor vehicles accidents are presented in this article. Preoperative suprapubic catheterization was initially carried out in all patients. Each patient then received one of three different techniques during the deferred time to surgical intervention: anterior sagittal transanorectal approach (ASTRA) for end-to-end urethral anastomosis, perineal approach for urethroplasty using buccal mucosa, and urethroplasty with preputial skin flap. The three techniques were successfully performed.
Discussion: In the initial management suprapubic cystostomy has been a good solution in urgent situations. Deferred urethroplasty is the procedure of choice for the definite treatment of posterior urethral distraction defects. The anterior sagittal transanorectal approach provides excellent exposure of the posterior urethra and retrovesicular region, and allows the surgeon to perform dissection under direct vision.
Conclusion: It's very important for the pediatric urologist to be familiar with the different techniques available in order to choose the best approach for each particular patient.
Keywords: Pediatric urethral trauma; Urethral injuries; Urethral reconstruction in children; Urethroplasty.
Copyright © 2017 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures






References
-
- Silber J.S., Flynn J.M., Koffler K.M., Dormans J.P., Drummond D.S. Analysis of the cause classification, and associated injuries of 166 consecutive pediatric pelvic fractures. J. Pediatr. Orthop. 2001;21:446–450. - PubMed
-
- Ismail N., Bellemare J.F., Mollitt D.L., DiScala C., Koeppel B., Tepas J. Death from pelvic fracture: children are different. J. Pediatr. Surg. 1996;31:82–85. - PubMed
-
- Tarman G.J., Kaplan G.W., Lerman S.L., Aleer I.M.M.C., Losasso B.E. Lower genitourinary injury and pelvic fractures in pediatric patients. Pediatr. Urol. 2002;59:123–126. - PubMed
-
- Orabi S., Badawy H., Saad A., Youssef M., Hanno A. Post-traumatic posterior urethral stricture in children: how to achieve a successful repair. J. Pediatr. Urol. 2008;4:290–294. - PubMed
-
- Mundy A.R., Andrich D.E. Urethral trauma. Part II: types of injuries and their management. BJU Int. 2011;180:630–650. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
