

Contrast Enhancement on Cone-Beam Breast-CT for Discrimination of Breast Cancer Immunohistochemical Subtypes
- PMID: 28946110
- PMCID: PMC5614638
- DOI: 10.1016/j.tranon.2017.08.010
Contrast Enhancement on Cone-Beam Breast-CT for Discrimination of Breast Cancer Immunohistochemical Subtypes
Abstract
Purpose: To evaluate whether contrast enhancement on cone-beam breast-CT (CBBCT) could aid in discrimination of breast cancer subtypes and receptor status.
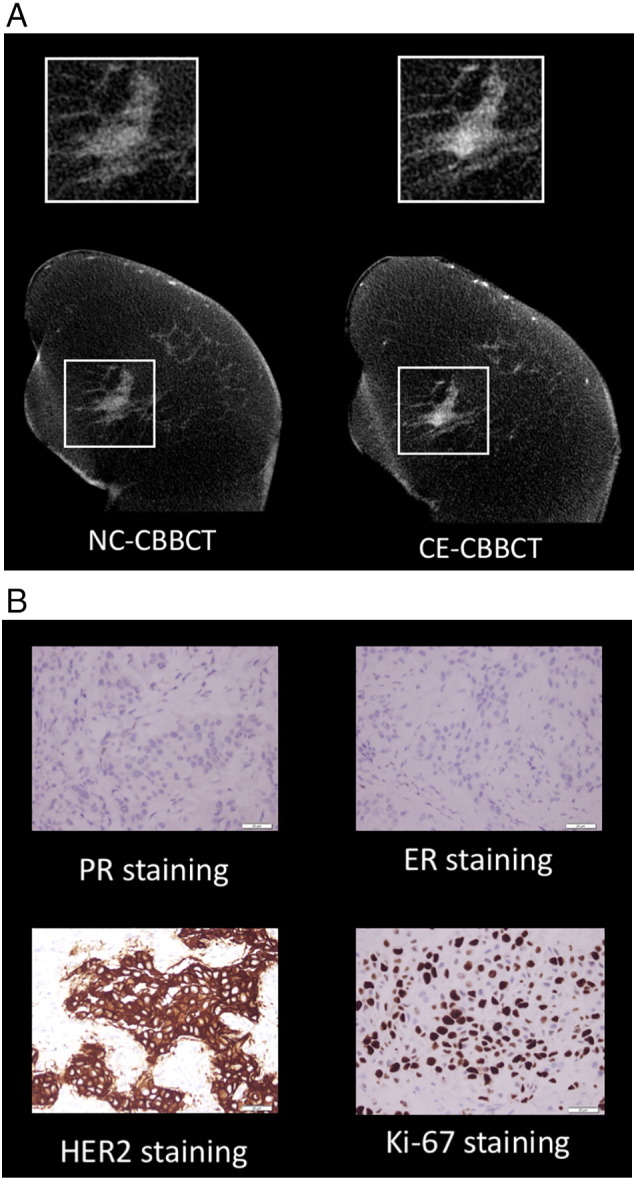
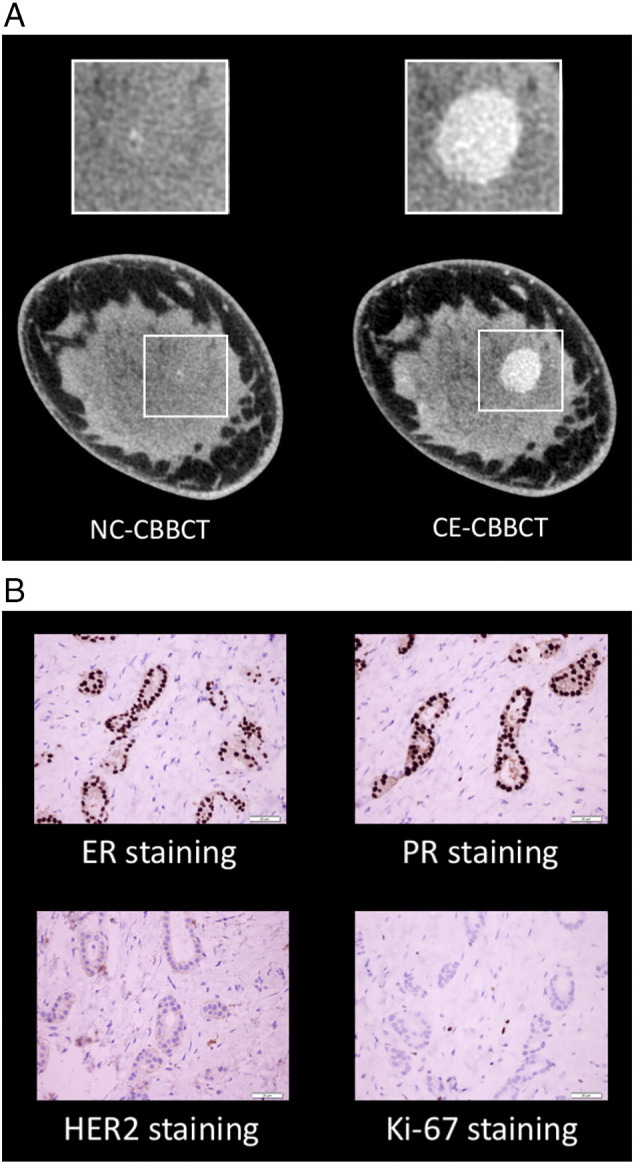
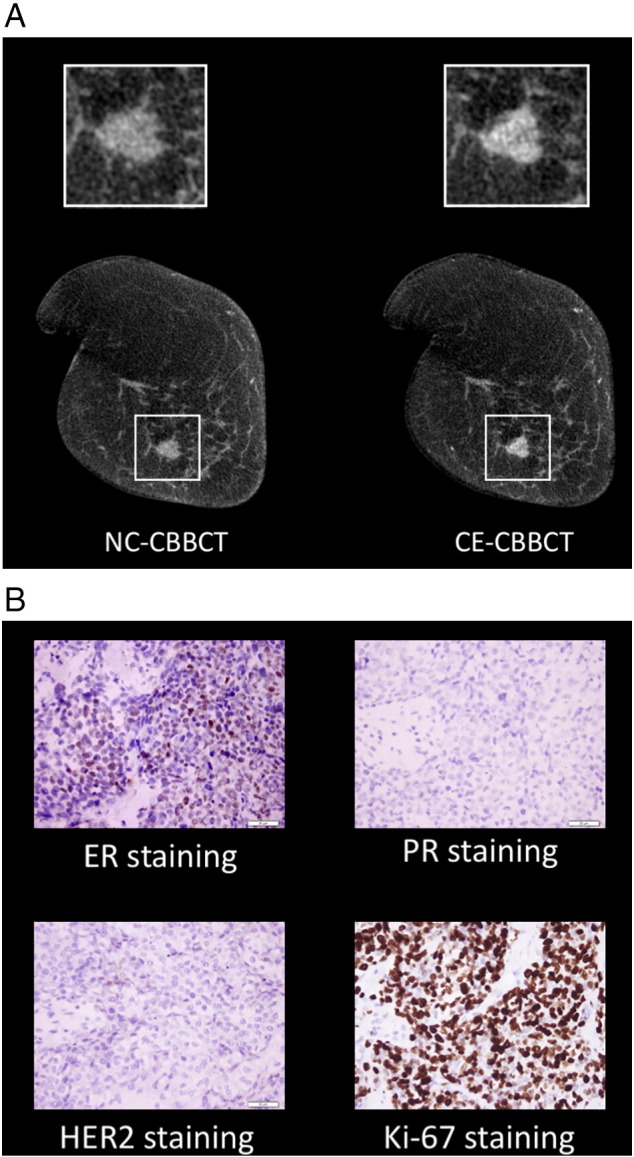
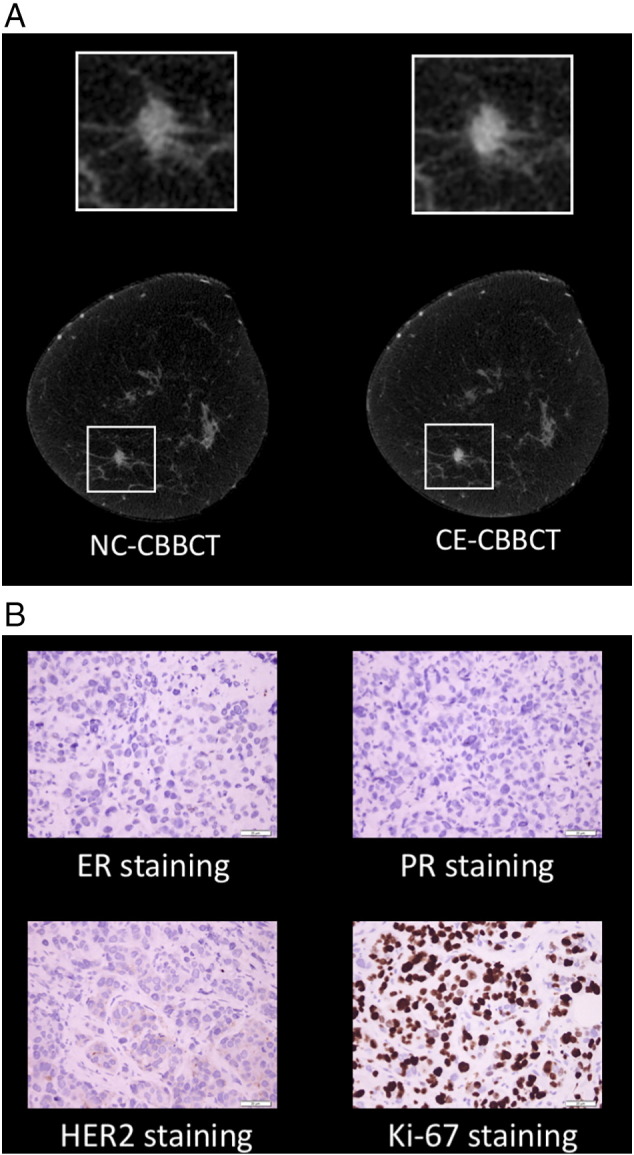
Methods: This study included female patients age >40 years with malignant breast lesions identified on contrast-enhanced CBBCT. Contrast enhancement of malignant breast lesions was standardized to breast fat tissue contrast enhancement. All breast lesions were approved via image-guided biopsy or surgery. Immunohistochemical staining was conducted for expression of estrogen (ER), progesterone (PR), human epidermal growth factor receptor-2 (HER2) and Ki-67 index. Contrast enhancement of breast lesions was correlated with immunohistochemical breast cancer subtypes (Luminal A, Luminal B, HER2 positive, triple negative), receptor status and Ki-67 expression.
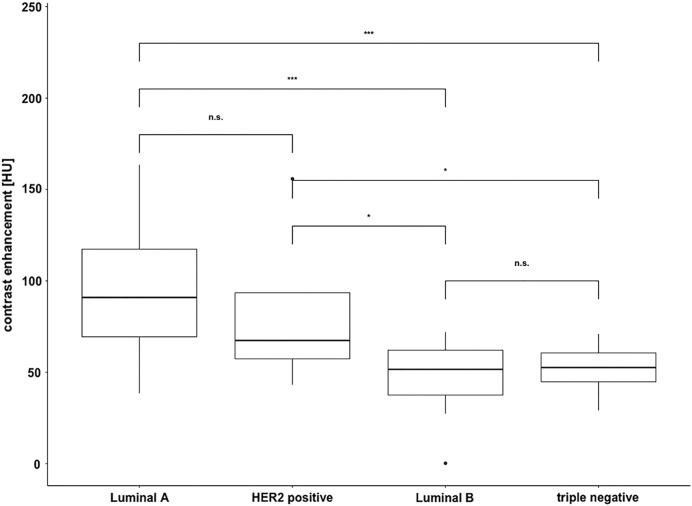
Results: Highest contrast enhancement was seen for Luminal A lesions (93.6 HU) compared to Luminal B lesions (47.6 HU, P=.002), HER2 positive lesions (83.5 HU, P=.359) and triple negative lesions (45.3 HU, P=.005). Contrast enhancement of HER2 positive lesions was higher than Luminal B lesions (P=.044) and triple negative lesions (P=.039). No significant difference was evident between Luminal B and triple negative lesions (P=.439). Lesions with high Ki-67 index showed lower contrast enhancement than those with low Ki-67 index (P=.0043). ER, PR and HER2 positive lesions demonstrated higher contrast enhancement than their receptor negative counterparts, although differences did not reach statistical significance (P=.1714; P=.3603; P=.2166).
Conclusions: Contrast enhancement of malignant breast lesions on CBBCT correlates with immunohistochemical subtype and proliferative potential. Thereby, CBBCT might aid in selecting individualized treatment strategies for breast cancer patients based on pre-operative imaging.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Contrast-enhanced cone-beam breast-CT: Analysis of optimal acquisition time for discrimination of breast lesion malignancy.Eur J Radiol. 2018 Feb;99:9-16. doi: 10.1016/j.ejrad.2017.12.003. Epub 2017 Dec 6. Eur J Radiol. 2018. PMID: 29362157
-
Breast MRI background parenchymal enhancement as an imaging bridge to molecular cancer sub-type.Eur J Radiol. 2019 Apr;113:148-152. doi: 10.1016/j.ejrad.2019.02.018. Epub 2019 Feb 15. Eur J Radiol. 2019. PMID: 30927939
-
Contrast-enhanced cone beam breast CT features of breast cancers: correlation with immunohistochemical receptors and molecular subtypes.Eur Radiol. 2021 Apr;31(4):2580-2589. doi: 10.1007/s00330-020-07277-8. Epub 2020 Oct 2. Eur Radiol. 2021. PMID: 33009590
-
Long-Term Outcomes of Immunohistochemically Defined Subtypes of Breast Cancer Less Than or Equal to 2 cm After Breast-Conserving Surgery.J Surg Res. 2019 Apr;236:288-299. doi: 10.1016/j.jss.2018.11.028. Epub 2018 Dec 27. J Surg Res. 2019. PMID: 30694768
-
The influence of receptor expression and clinical subtypes on baseline [18F]FDG uptake in breast cancer: systematic review and meta-analysis.EJNMMI Res. 2023 Jan 23;13(1):5. doi: 10.1186/s13550-023-00953-y. EJNMMI Res. 2023. PMID: 36689007 Free PMC article. Review.
Cited by
-
Cone-beam breast CT features associated with HER2/neu overexpression in patients with primary breast cancer.Eur Radiol. 2020 May;30(5):2731-2739. doi: 10.1007/s00330-019-06587-w. Epub 2020 Jan 3. Eur Radiol. 2020. PMID: 31900700
-
Correlation between contrast-enhanced cone-beam breast computed tomography features and prognostic staging in breast cancer.Br J Radiol. 2022 Apr 1;95(1132):20210466. doi: 10.1259/bjr.20210466. Epub 2022 Jan 7. Br J Radiol. 2022. PMID: 34930038 Free PMC article.
-
Breast Cancer Screening: Opportunities and Challenges with Fully 3D Tomographic X-Ray Imaging.Bridge (Wash D C). 2022 Spring;52(1):33-42. Epub 2022 Mar 28. Bridge (Wash D C). 2022. PMID: 35431425 Free PMC article. No abstract available.
-
The feasibility of contrast-enhanced spectral mammography immediately after contrast-enhanced CT.Radiol Phys Technol. 2019 Sep;12(3):277-282. doi: 10.1007/s12194-019-00518-6. Epub 2019 Jun 5. Radiol Phys Technol. 2019. PMID: 31165975
-
Towards 4D dedicated breast CT perfusion imaging of cancer: development and validation of computer simulated images.Phys Med Biol. 2019 Dec 13;64(24):245004. doi: 10.1088/1361-6560/ab55ac. Phys Med Biol. 2019. PMID: 31703216 Free PMC article.
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74–108. - PubMed
-
- Perou CM, Sorlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, Pollack JR, Ross DT, Johnsen H, Akslen LA. Molecular portraits of human breast tumours. Nature. 2000;406(6797):747–752. - PubMed
-
- Nielsen TO, Hsu FD, Jensen K, Cheang M, Karaca G, Hu Z, Hernandez-Boussard T, Livasy C, Cowan D, Dressler L. Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin Cancer Res. 2004;10(16):5367–5374. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
