

Comparison of Minimal Residual Disease Detection by Multiparameter Flow Cytometry, ASO-qPCR, Droplet Digital PCR, and Deep Sequencing in Patients with Multiple Myeloma Who Underwent Autologous Stem Cell Transplantation
- PMID: 28946710
- PMCID: PMC5664006
- DOI: 10.3390/jcm6100091
Comparison of Minimal Residual Disease Detection by Multiparameter Flow Cytometry, ASO-qPCR, Droplet Digital PCR, and Deep Sequencing in Patients with Multiple Myeloma Who Underwent Autologous Stem Cell Transplantation
Erratum in
-
Takamatsu, H. Comparison of Minimal Residual Disease Detection by Multiparameter Flow Cytometry, ASO-qPCR, Droplet Digital PCR, and Deep Sequencing in Patients with Multiple Myeloma Who Underwent Autologous Stem Cell Transplantation. J. Clin. Med. 2017, 6, 91.J Clin Med. 2017 Nov 20;6(11):106. doi: 10.3390/jcm6110106. J Clin Med. 2017. PMID: 29156604 Free PMC article.
Abstract
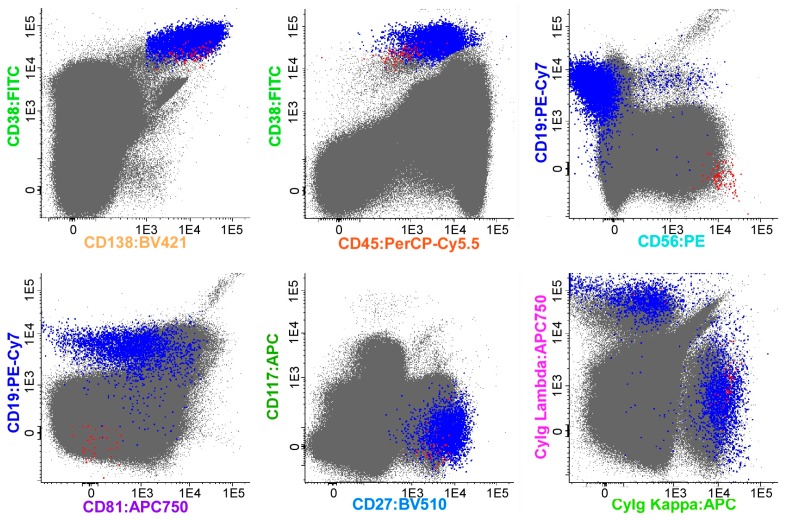
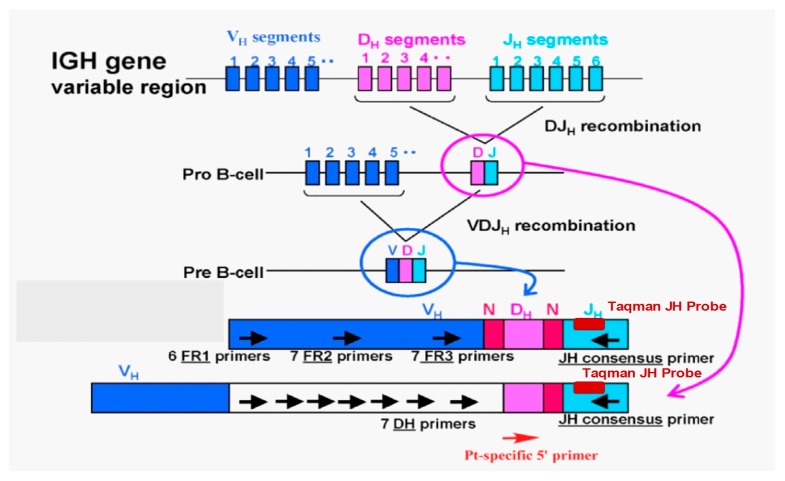
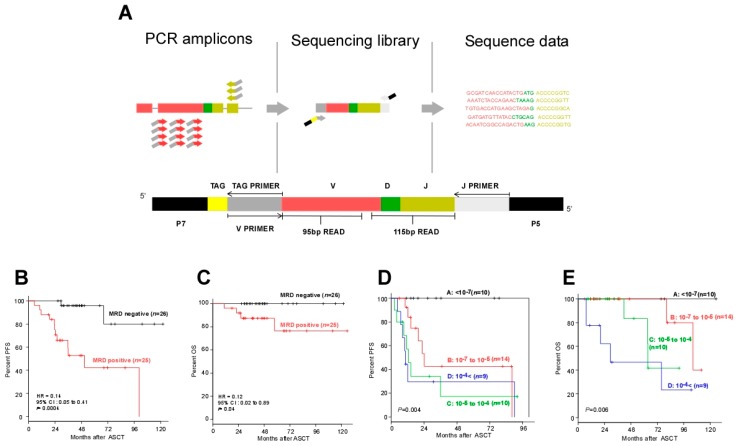
Multiple myeloma (MM) is a hematological malignancy with a poor prognosis, characterized by clonal proliferation of plasma cells in the bone marrow (BM). Relapse due to undetected minimal residual disease (MRD) is the leading cause of death among patients with MM. This review summarizes the methods and prognostic value of MRD assessment in BM and autografts from MM patients who underwent autologous stem cell transplantation (ASCT) by multiparameter flow cytometry (MFC), allele-specific oligonucleotide real-time quantitative PCR (ASO-qPCR), droplet digital PCR (ddPCR), and next-generation sequencing (NGS)-based detection methods. MRD assessment using NGS-based approaches has clear prognostic value and better sensitivity compared to traditional methods.
Keywords: allele-specific oligonucleotide-PCR; droplet digital PCR; minimal residual disease; multiple myeloma; next-generation sequencing.
Conflict of interest statement
The author received research funding from Takeda and Fujimoto, and honoraria from Celgene and Janssen.
Figures
References
-
- San Miguel J.F., Schlag R., Khuageva N.K., Dimopoulos M.A., Shpilberg O., Kropff M., Spicka I., Petrucci M.T., Palumbo A., Samoilova O.S., et al. Bortezomib plus melphalan and prednisone for initial treatment of multiple myeloma. N. Engl. J. Med. 2008;359:906–917. doi: 10.1056/NEJMoa0801479. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
