

Managing Complications in Abdominoplasty: A Literature Review
- PMID: 28946731
- PMCID: PMC5621815
- DOI: 10.5999/aps.2017.44.5.457
Managing Complications in Abdominoplasty: A Literature Review
Abstract
Background: Abdominoplasty, with or without liposuction, is among the most frequently performed aesthetic procedures. Its main objective is to improve the body contour by means of excising redundant skin and fat tissue. Although abdominoplasty is considered a safe procedure with high satisfaction rates, intraoperative and postoperative complications can become a challenge for the surgical team. The aim of this article is to offer a synopsis of the most common complications arising after abdominoplasty, along with evidence-based guidelines about how to prevent and treat them.
Methods: A systematic MEDLINE search strategy was designed using appropriate Medical Subject Headings (MeSH) terms, and references were scanned for further relevant articles.
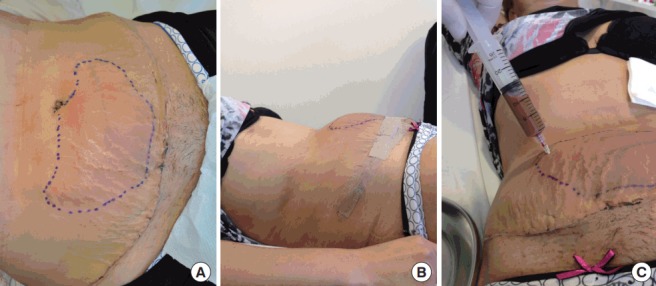
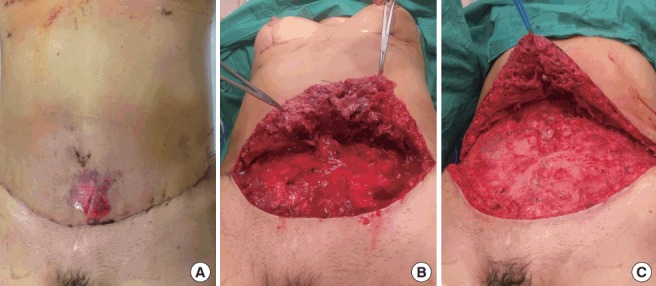
Results: According to the published case series, local complications are considerably more common than complications with systemic repercussions. Approximately 10% to 20% of patients suffer a local complication following abdominoplasty, while fewer than 1% suffer a systemic complication. Prevention and management strategies are critically discussed for complications including seroma, haematoma, infection, skin necrosis, suture extrusions, hypertrophic scars, neurological symptoms, umbilical anomalies, deep venous thrombosis and pulmonary thromboembolism, respiratory distress, and death.
Conclusions: The complications of abdominoplasty vary in severity and in the impact they have on the aesthetic outcomes. Recommendations for prevention and management are based on various levels of evidence, with a risk of observer bias. However, most complications can be treated appropriately following the current standards, with satisfactory results.
Keywords: Abdominoplasty; Complications; Cosmetic techniques; Lipectomy; Reconstructive surgical procedure; Surgery, plastic.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures








References
-
- International Society of Aesthetic Plastic Surgery . International study on aesthetic/cosmetic procedures performed in 2013. Hanover: International Society of Aesthetic Plastic Surgery; 2014.
-
- Kelly HA. Excision of the fat of the abdominal wall lipectomy. Surg Gynecol Obstet. 1910;10:229–31.
-
- Vernon S. Umbilical transplantation upward and abdominal contouring in lipectomy. Am J Surg. 1957;94:490–2. - PubMed
-
- Pitanguy I. Abdominal lipectomy: an approach to it through an analysis of 300 consecutive cases. Plast Reconstr Surg. 1967;40:384–91.
-
- Grazer FM. Abdominoplasty. Plast Reconstr Surg. 1973;51:617–23. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources