

A Whole Blood Molecular Signature for Acute Myocardial Infarction
- PMID: 28947747
- PMCID: PMC5612952
- DOI: 10.1038/s41598-017-12166-0
A Whole Blood Molecular Signature for Acute Myocardial Infarction
Abstract
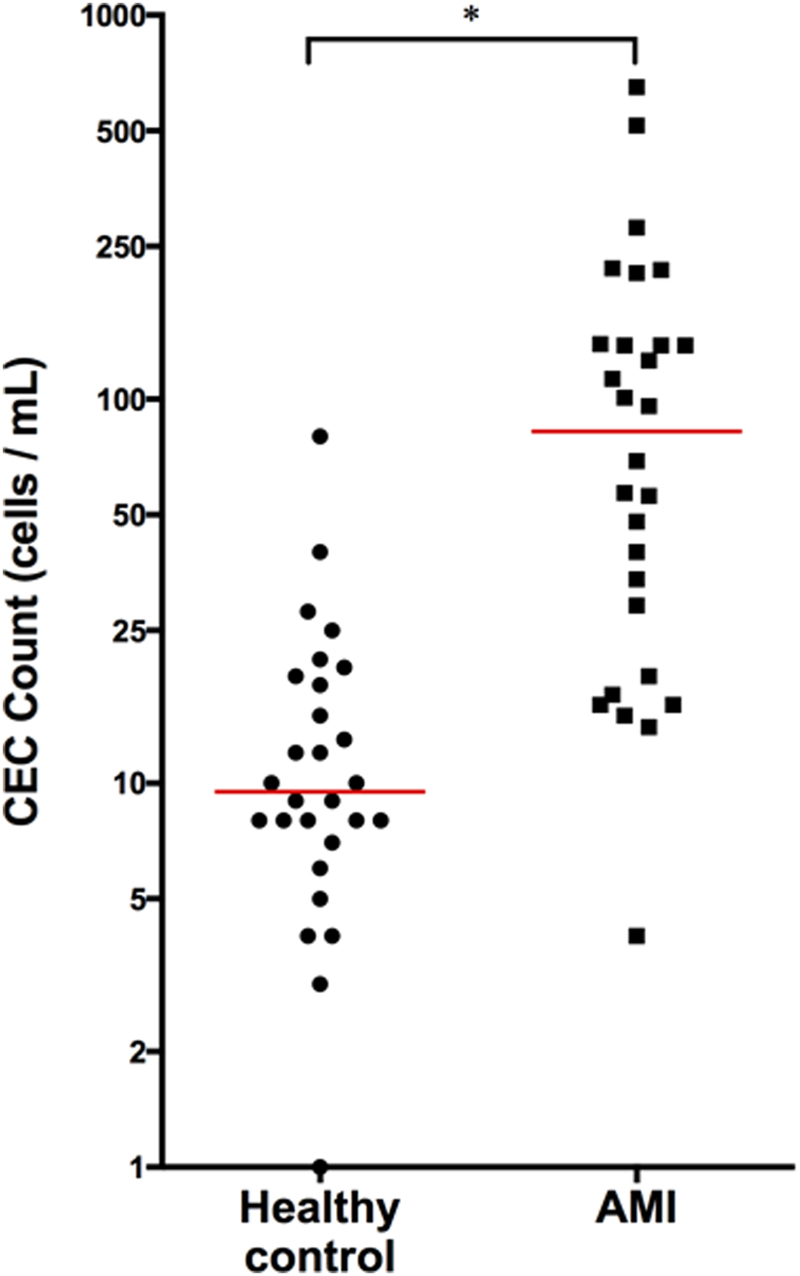
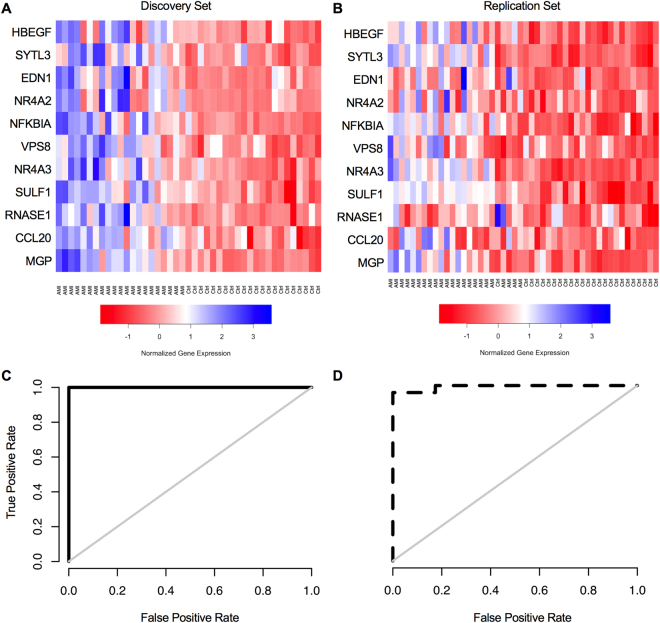
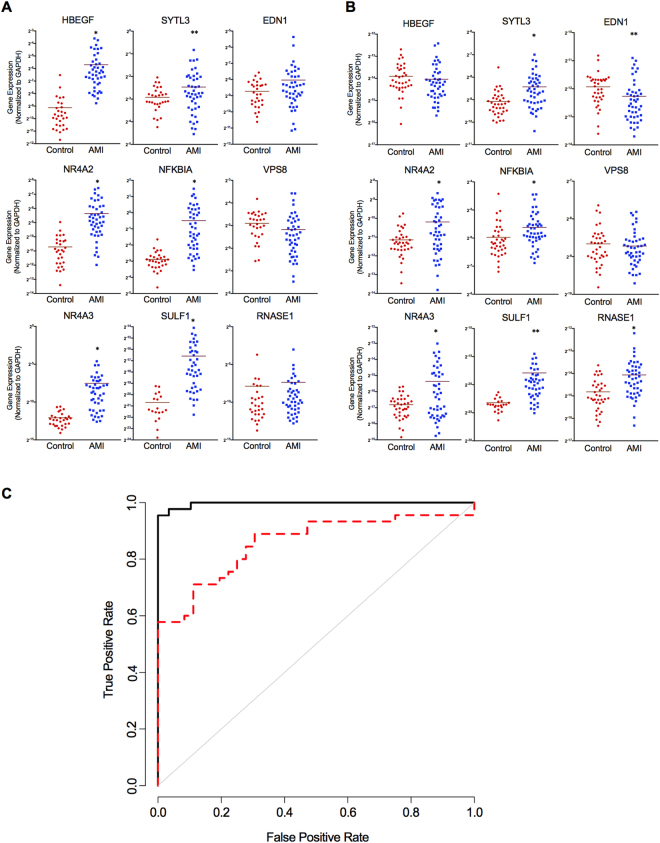
Chest pain is a leading reason patients seek medical evaluation. While assays to detect myocyte death are used to diagnose a heart attack (acute myocardial infarction, AMI), there is no biomarker to indicate an impending cardiac event. Transcriptional patterns present in circulating endothelial cells (CEC) may provide a window into the plaque rupture process and identify a proximal biomarker for AMI. Thus, we aimed to identify a transcriptomic signature of AMI present in whole blood, but derived from CECs. Candidate genes indicative of AMI were nominated from microarray of enriched CEC samples, and then verified for detectability and predictive potential via qPCR in whole blood. This signature was validated in an independent cohort. Our findings suggest that a whole blood CEC-derived molecular signature identifies patients with AMI and sets the framework to potentially identify the earlier stages of an impending cardiac event when used in concert with clinical history and other diagnostics where conventional biomarkers indicative of myonecrosis remain undetected.
Conflict of interest statement
E.D.M., E.J.T., H.W., T.A.J. and M.C.C. are listed as co-inventors on a pending patent for the predictive analysis of myocardial infarction. Biologic Dynamics holds a patent for circulating microparticle isolation.
Figures
Similar articles
-
Detection and validation of circulating endothelial cells, a blood-based diagnostic marker of acute myocardial infarction.PLoS One. 2013;8(3):e58478. doi: 10.1371/journal.pone.0058478. Epub 2013 Mar 4. PLoS One. 2013. PMID: 23484031 Free PMC article.
-
MiR-103a targeting Piezo1 is involved in acute myocardial infarction through regulating endothelium function.Cardiol J. 2016;23(5):556-562. doi: 10.5603/CJ.a2016.0056. Epub 2016 Aug 12. Cardiol J. 2016. PMID: 27515482
-
Circulating Endothelial Cells and Endothelial Function Predict Major Adverse Cardiac Events and Early Adverse Left Ventricular Remodeling in Patients With ST-Segment Elevation Myocardial Infarction.J Interv Cardiol. 2016 Feb;29(1):89-98. doi: 10.1111/joic.12269. J Interv Cardiol. 2016. PMID: 26864952 Free PMC article.
-
Potential of lipoproteins as biomarkers in acute myocardial infarction.Anatol J Cardiol. 2017 Jul;18(1):68-74. doi: 10.14744/AnatolJCardiol.2017.7403. Anatol J Cardiol. 2017. PMID: 28680021 Free PMC article. Review.
-
Rupture of the left ventricular free wall during acute myocardial infarction: analysis of 138 necropsy patients and comparison with 50 necropsy patients with acute myocardial infarction without rupture.Am J Cardiol. 1988 Nov 1;62(13):847-59. doi: 10.1016/0002-9149(88)90881-8. Am J Cardiol. 1988. PMID: 3052010 Review.
Cited by
-
Effect of SYTL3-SLC22A3 Variants, Their Haplotypes, and G × E Interactions on Serum Lipid Levels and the Risk of Coronary Artery Disease and Ischaemic Stroke.Front Cardiovasc Med. 2021 Aug 12;8:713068. doi: 10.3389/fcvm.2021.713068. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34458338 Free PMC article.
-
Identification of shared fatty acid metabolism related signatures in dilated cardiomyopathy and myocardial infarction.Future Sci OA. 2023 Mar 28;9(3):FSO847. doi: 10.2144/fsoa-2023-0008. eCollection 2023 Mar. Future Sci OA. 2023. PMID: 37056578 Free PMC article.
-
Identification of Key Genes Involved in Acute Myocardial Infarction by Comparative Transcriptome Analysis.Biomed Res Int. 2020 Oct 6;2020:1470867. doi: 10.1155/2020/1470867. eCollection 2020. Biomed Res Int. 2020. PMID: 33083450 Free PMC article.
-
Identification of mitochondria-related gene biomarkers associated with immune infiltration in acute myocardial infarction.iScience. 2024 Jun 14;27(7):110275. doi: 10.1016/j.isci.2024.110275. eCollection 2024 Jul 19. iScience. 2024. PMID: 39040073 Free PMC article.
-
Novel diagnostic biomarkers related to necroptosis and immune infiltration landscape in acute myocardial infarction.PeerJ. 2024 Feb 26;12:e17044. doi: 10.7717/peerj.17044. eCollection 2024. PeerJ. 2024. PMID: 38426147 Free PMC article.
References
-
- WHO. World Health Organization. Global status report on non-communicable diseases. (2014).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
