

Clinical evaluation of macrophages in cancer: role in treatment, modulation and challenges
- PMID: 28948324
- PMCID: PMC11028704
- DOI: 10.1007/s00262-017-2065-0
Clinical evaluation of macrophages in cancer: role in treatment, modulation and challenges
Abstract
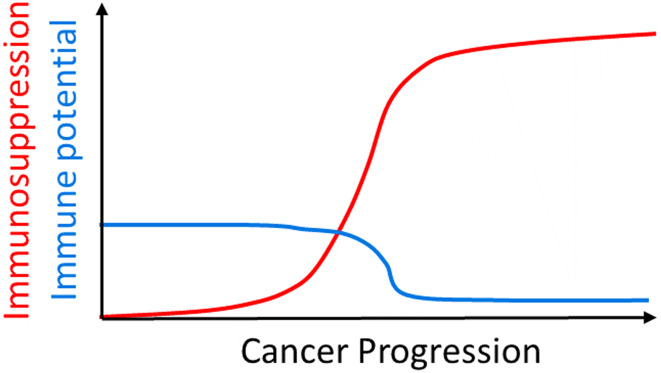
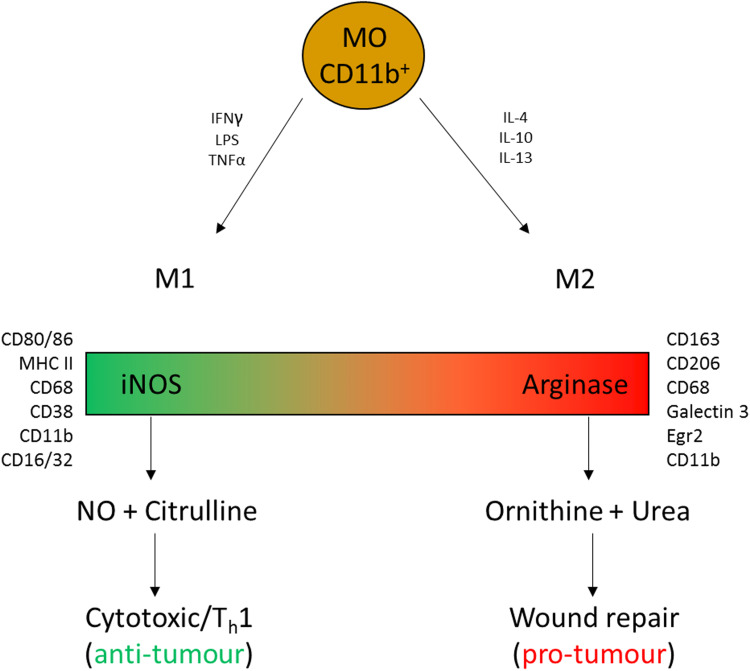
The focus of immunotherapeutics has been placed firmly on anti-tumour T cell responses. Significant progress has been made in the treatment of both local and systemic malignancies, but low response rates and rising toxicities are limiting this approach. Advancements in the understanding of tumour immunology are opening up a new range of therapeutic targets, including immunosuppressive factors in the tumour microenvironment. Macrophages are a heterogeneous group of cells that have roles in innate and adaptive immunity and tissue repair, but become co-opted by tumours to support tumour growth, survival, metastasis and immunosuppression. Macrophages also support tumour resistance to conventional therapy. In preclinical models, interference with macrophage migration, macrophage depletion and macrophage re-education have all been shown to reduce tumour growth and support anti-tumour immune responses. Here we discuss the role of macrophages in prognosis and sensitivity to therapy, while examining the significant progress which has been made in modulating the behaviour of these cells in cancer patients.
Keywords: Cancer; Immunology; Immunotherapy; Macrophage.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
Harnessing the innate immune system by revolutionizing macrophage-mediated cancer immunotherapy.J Biosci. 2024;49:68 63. doi: 10.1007/s12038-024-00441-y. J Biosci. 2024. PMID: 38864238 Free PMC article. Review.
-
Macrophage-Mediated Subversion of Anti-Tumour Immunity.Cells. 2019 Jul 19;8(7):747. doi: 10.3390/cells8070747. Cells. 2019. PMID: 31331034 Free PMC article. Review.
-
The Multifaceted Role of Macrophages in Oncolytic Virotherapy.Viruses. 2021 Aug 9;13(8):1570. doi: 10.3390/v13081570. Viruses. 2021. PMID: 34452439 Free PMC article. Review.
-
Immunology in the clinic review series; focus on cancer: tumour-associated macrophages: undisputed stars of the inflammatory tumour microenvironment.Clin Exp Immunol. 2012 Feb;167(2):195-205. doi: 10.1111/j.1365-2249.2011.04515.x. Clin Exp Immunol. 2012. PMID: 22235995 Free PMC article. Review.
-
Molecular Repolarisation of Tumour-Associated Macrophages.Molecules. 2018 Dec 20;24(1):9. doi: 10.3390/molecules24010009. Molecules. 2018. PMID: 30577495 Free PMC article. Review.
Cited by
-
Melanoma-conditioned medium promotes cytotoxic immune responses by murine bone marrow-derived monocytes despite their expression of 'M2' markers.Cancer Immunol Immunother. 2019 Sep;68(9):1455-1465. doi: 10.1007/s00262-019-02381-1. Epub 2019 Aug 23. Cancer Immunol Immunother. 2019. PMID: 31444606 Free PMC article.
-
Role of Tumor-Associated Macrophages in the Clinical Course of Pancreatic Neuroendocrine Tumors (PanNETs).Clin Cancer Res. 2019 Apr 15;25(8):2644-2655. doi: 10.1158/1078-0432.CCR-18-1401. Epub 2019 Jan 22. Clin Cancer Res. 2019. PMID: 30670493 Free PMC article.
-
An immunosuppressive macrophage profile attenuates the prognostic impact of CD20-positive B cells in human soft tissue sarcoma.Cancer Immunol Immunother. 2019 Jun;68(6):927-936. doi: 10.1007/s00262-019-02322-y. Epub 2019 Mar 16. Cancer Immunol Immunother. 2019. PMID: 30879106 Free PMC article.
-
Cellular backpacks for macrophage immunotherapy.Sci Adv. 2020 Apr 29;6(18):eaaz6579. doi: 10.1126/sciadv.aaz6579. eCollection 2020 May. Sci Adv. 2020. PMID: 32494680 Free PMC article.
-
Differential association of CD68+ and CD163+ macrophages with macrophage enzymes, whole tumour gene expression and overall survival in advanced melanoma.Br J Cancer. 2020 Nov;123(10):1553-1561. doi: 10.1038/s41416-020-01037-7. Epub 2020 Aug 26. Br J Cancer. 2020. PMID: 32843682 Free PMC article.
References
-
- Hassel JC, Heinzerling L, Aberle J, Bahr O, Eigentler TK, Grimm MO, Grunwald V, Leipe J, Reinmuth N, Tietze JK, Trojan J, Zimmer L, Gutzmer R. Combined immune checkpoint blockade (anti-PD-1/anti-CTLA-4): evaluation and management of adverse drug reactions. Cancer Treat Rev. 2017;57:36–49. doi: 10.1016/j.ctrv.2017.05.003. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
