

Prevalence of Prediabetes and Undiagnosed Diabetes in Patients with HFpEF and HFrEF and Associated Clinical Outcomes
- PMID: 28948430
- PMCID: PMC5730631
- DOI: 10.1007/s10557-017-6754-x
Prevalence of Prediabetes and Undiagnosed Diabetes in Patients with HFpEF and HFrEF and Associated Clinical Outcomes
Abstract
Purpose: The prevalence and consequences of prediabetic dysglycemia and undiagnosed diabetes is unknown in patients with heart failure (HF) and preserved ejection fraction (HFpEF) and has not been compared to heart failure and reduced ejection fraction (HFrEF).
Methods: We examined the prevalence and outcomes associated with normoglycemia, prediabetic dysglycemia and diabetes (diagnosed and undiagnosed) among individuals with a baseline glycated hemoglobin (hemoglobin A1c, HbA1c) measurement stratified by HFrEF or HFpEF in the Candesartan in Heart failure Assessment of Reduction in Mortality and morbidity programme (CHARM). We studied the primary outcome of HF hospitalization or cardiovascular (CV) death, and all-cause death, and estimated hazard ratios (HR) by use of multivariable Cox regression models.
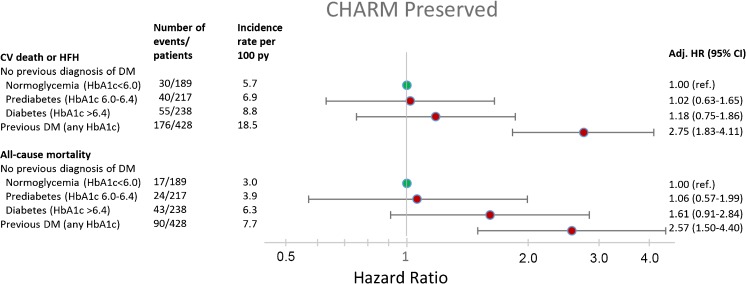
Results: HbA1c was measured at baseline in CHARM patients enrolled in the USA and Canada and was available in 1072/3023 (35%) of patients with HFpEF and 1578/4576 (34%) patients with HFrEF. 18 and 16% had normoglycemia (HbA1c < 6.0), 20 and 22% had prediabetes (HbA1c 6.0-6.4), respectively. Finally among patients with HFpEF 22% had undiagnosed diabetes (HbA1c > 6.4), and 40% had known diabetes (any HbA1c), with corresponding prevalence among HFrEF patients being 26 and 35%. The rates of both clinical outcomes of interest were higher in patients with undiagnosed diabetes and prediabetes, compared to normoglycemic patients, irrespective of HF subtype, and in general higher among HFrEF patients. For the primary composite outcome among HFpEF patients, the HRs were 1.02 (95% CI 0.63-1.65) for prediabetes, HR 1.18 (0.75-1.86) for undiagnosed diabetes and 2.75 (1.83-4.11) for known diabetes, respectively, p value for trend across groups < 0.001. Dysglycemia was also associated with worse outcomes in HFrEF.
Conclusions: These findings confirm the remarkably high prevalence of dysglycemia in heart failure irrespective of ejection fraction phenotype, and demonstrate that dysglycemia is associated with a higher risk of adverse clinical outcomes, even before the diagnosis of diabetes and institution of glucose lowering therapy in patients with HFpEF as well as HFrEF.
Keywords: Diabetes; Dysglycemia; Heart failure; Heart failure and preserved ejection fraction; Prognosis.
Conflict of interest statement
Conflict of Interest
Drs. Kristensen, Jhund and Lee report no relevant conflict of interests. All other authors have received honoraria as steering committee members of CHARM from AstraZeneca.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Figures

References
-
- MacDonald MR, Petrie MC, Varyani F, et al. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur Heart J. 2008;29:1377–1385. doi: 10.1093/eurheartj/ehn153. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
