

Acetabular Reconstruction With Femoral Head Autograft After Intraarticular Resection of Periacetabular Tumors is Durable at Short-term Followup
- PMID: 28948491
- PMCID: PMC5670074
- DOI: 10.1007/s11999-017-5505-4
Acetabular Reconstruction With Femoral Head Autograft After Intraarticular Resection of Periacetabular Tumors is Durable at Short-term Followup
Abstract
Background: Pelvic reconstruction after periacetabular tumor resection is technically difficult and characterized by a high complication rate. Although endoprosthetic replacement can result in immediate postoperative functional recovery, biologic reconstructions with autograft may provide an enhanced prognosis in patients with long-term survival; however, little has been published regarding this approach. We therefore wished to evaluate whether whole-bulk femoral head autograft that is not contaminated by tumor can be used to reconstruct segmental bone defects after intraarticular resection of periacetabular tumors.
Questions/purposes: In a pilot study, we evaluated (1) local tumor control, (2) complications, and (3) postoperative function as measured by the Musculoskeletal Tumor Society score.
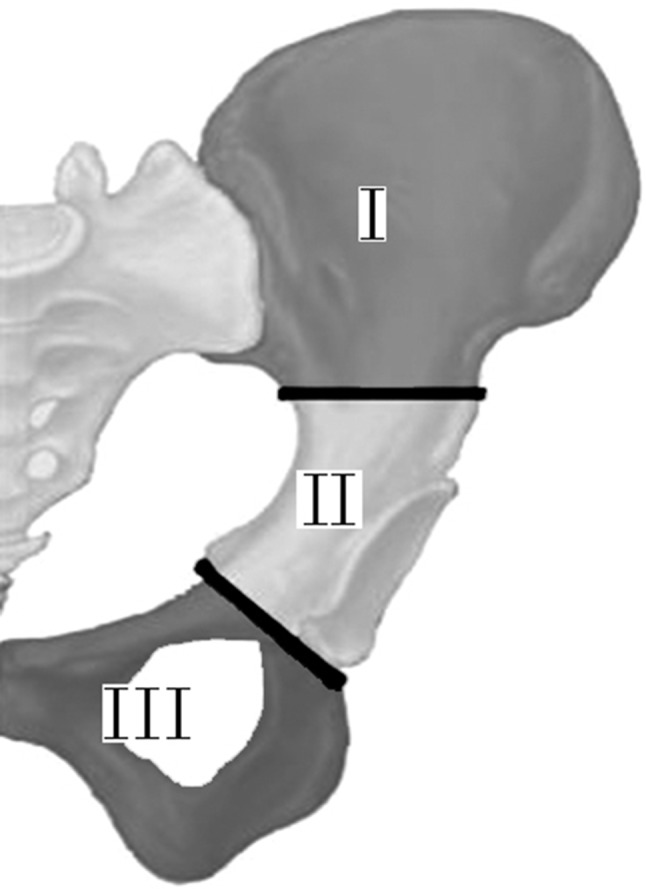
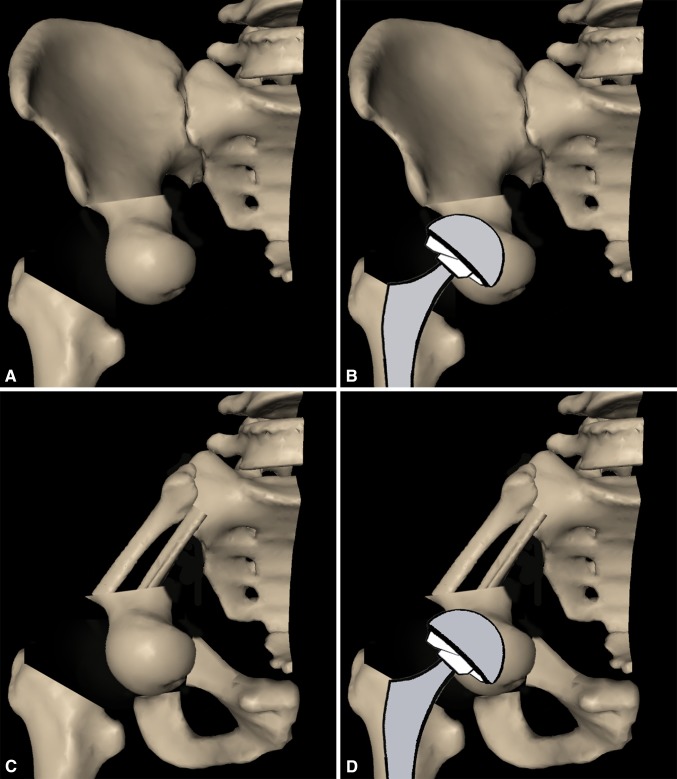
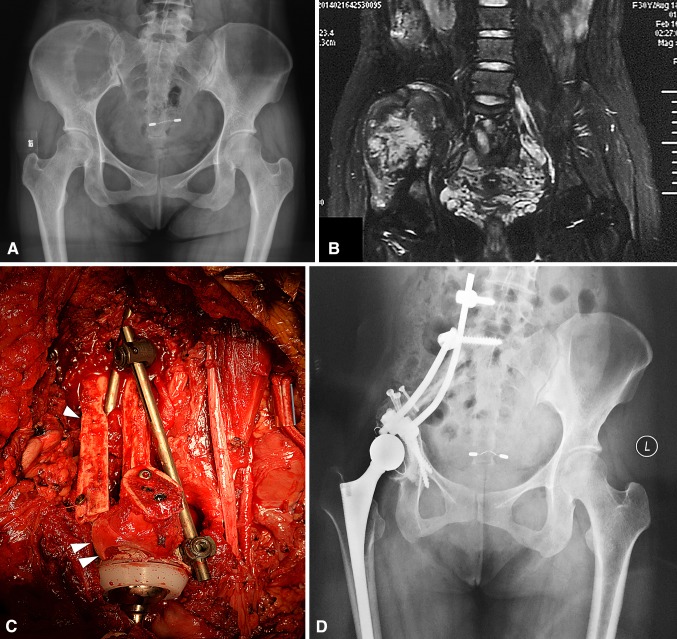
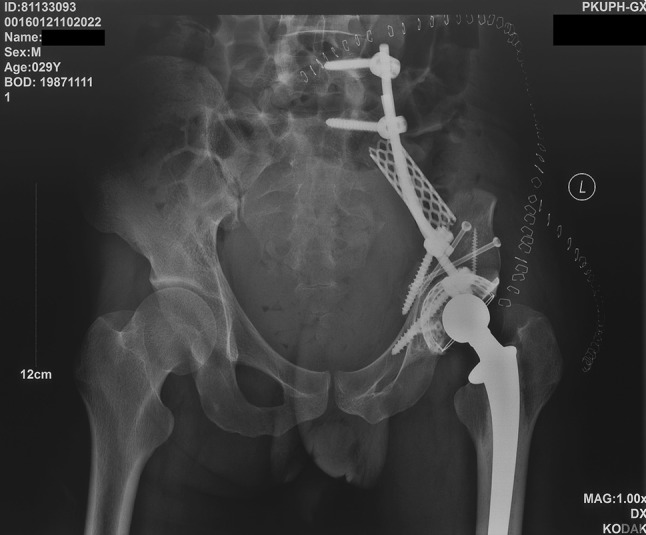
Methods: Between 2009 and 2015, we treated 13 patients with periacetabular malignant or aggressive benign tumors with en bloc resection, bulk femoral head autograft, and cemented THA (with or without a titanium acetabular reconstruction cup), and all were included for analysis here. During that time, the general indications for this approach were (1) patients anticipated to have a good oncologic prognosis and adequate surgical margins to allow this approach, (2) patients whose pelvic bone defects did not exceed two types (Types I + II or Types II + III as defined by Enneking and Dunham), and (3) patients whose medical insurance would not cover what otherwise might have been a pelvic tumor prosthesis. During this period, another 91 patients were treated with pelvic prosthetic replacement, which was our preferred approach. Median followup in this study was 36 months (range, 24-99 months among surviving patients; one patient died 8 months after surgery); no patients were lost to followup. Bone defects were Types II + III in five patients, and Types I + II in eight. After intraarticular resection, ipsilateral femoral head autograft combined with THA was used to reconstruct the segmental bone defect of the acetabulum. In patients with Types I + II resections, the connection between the sacrum and the acetabulum was reestablished with a fibular autograft or a titanium cage filled with dried bone-allograft particles which was enhanced by using a pedicle screw and rod system. Functional evaluation was done in 11 patients who remained alive and maintained the femoral head autograft at final followup; one other patient received secondary resection involving removal of the femoral head autograft and internal fixation, and was excluded from functional evaluation. Endpoints were assessed by chart review.
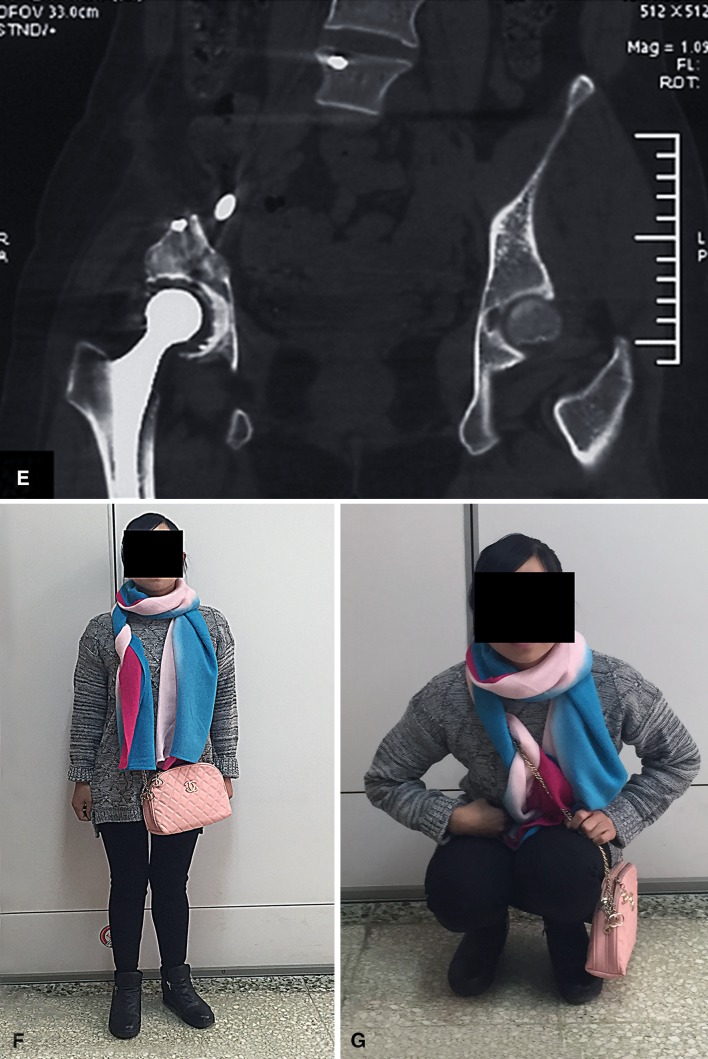
Results: Two patients experienced local tumor recurrence. Finally, eight patients did not show signs of the disease, one patient died of disease for local and distant tumor relapse, and four patients survived, but still had the disease. Three of these four patients had distant metastases without local recurrence and one had local control after secondary resection but still experienced system relapse. We observed the following complications: hematoma (one patient; treated surgically with hematoma clearance), delayed wound healing (one patient; treated by débridement), deep vein thrombosis (one patient), and hip dislocation (one patient; treated with open reduction). The median 1993 Musculoskeletal Tumor Society score was 83% (25 of 30 points; range, 19-29 points), and all patients were community ambulators; one used a cane, three used a walker, and nine did not use any assistive devices.
Conclusions: In this small series at short-term followup, we found that reconstruction of segmental bone defects after intraarticular resection of periacetabular tumors with femoral head autograft does not appear to impede local tumor control; complications were in the range of what might be expected in a series of large pelvic reconstructions, and postoperative function was generally good.
Level of evidence: Level IV, therapeutic study.
Figures
Similar articles
-
Upshifting the Ipsilateral Proximal Femur May Provide Satisfactory Reconstruction of Periacetabular Pelvic Bone Defects After Tumor Resection.Clin Orthop Relat Res. 2018 Sep;476(9):1762-1770. doi: 10.1007/s11999.0000000000000165. Clin Orthop Relat Res. 2018. PMID: 30794213 Free PMC article.
-
LUMiC® Endoprosthetic Reconstruction After Periacetabular Tumor Resection: Short-term Results.Clin Orthop Relat Res. 2017 Mar;475(3):686-695. doi: 10.1007/s11999-016-4805-4. Clin Orthop Relat Res. 2017. PMID: 27020434 Free PMC article.
-
Is a Modular Pedicle-hemipelvic Endoprosthesis Durable at Short Term in Patients Undergoing Enneking Type I + II Tumor Resections With or Without Sacroiliac Involvement?Clin Orthop Relat Res. 2018 Sep;476(9):1751-1761. doi: 10.1007/s11999.0000000000000121. Clin Orthop Relat Res. 2018. PMID: 30794212 Free PMC article.
-
Does adding sacroiliac (type IV) resection to periacetabular (type II) resection increase complications or provide worse clinical outcomes? An institutional experience and systematic review.Surg Oncol. 2024 Oct;56:102116. doi: 10.1016/j.suronc.2024.102116. Epub 2024 Aug 8. Surg Oncol. 2024. PMID: 39128439
-
The outcome of type 1 pelvic resection and reconstruction with pedicle screw-rod system without bone grafting in malignant pelvic tumour: A case series and short term review.J Orthop Surg (Hong Kong). 2022 May-Aug;30(2):10225536221119510. doi: 10.1177/10225536221119510. J Orthop Surg (Hong Kong). 2022. PMID: 35982537 Review.
Cited by
-
Reconstruction with customized, 3D-printed prosthesis after resection of periacetabular Ewing's sarcoma in children using "triradiate cartilage-based" surgical strategy:a technical note.J Orthop Translat. 2021 Mar 26;28:108-117. doi: 10.1016/j.jot.2020.12.006. eCollection 2021 May. J Orthop Translat. 2021. PMID: 33868923 Free PMC article.
-
Short-term Preoperative Denosumab With Surgery in Unresectable or Recurrent Giant Cell Tumor of Bone.Orthop Surg. 2019 Dec;11(6):1101-1108. doi: 10.1111/os.12561. Epub 2019 Nov 25. Orthop Surg. 2019. PMID: 31762217 Free PMC article.
-
Does Adding Femoral Lengthening at the Time of Rotation Hip Transposition After Periacetabular Tumor Resection Allow for Restoration of Limb Length and Function? Interim Results of a Modified Hip Transposition Procedure.Clin Orthop Relat Res. 2021 Jul 1;479(7):1521-1530. doi: 10.1097/CORR.0000000000001653. Clin Orthop Relat Res. 2021. PMID: 33534263 Free PMC article.
-
3D-Printed Prosthesis with an Articular Interface for Anatomical Acetabular Reconstruction After Type I + II (+ III) Internal Hemipelvectomy: Clinical Outcomes and Finite Element Analysis.J Bone Joint Surg Am. 2025 Jan 15;107(2):184-195. doi: 10.2106/JBJS.23.01462. Epub 2024 Oct 15. J Bone Joint Surg Am. 2025. PMID: 39729975 Free PMC article.
-
Upshifting the Ipsilateral Proximal Femur May Provide Satisfactory Reconstruction of Periacetabular Pelvic Bone Defects After Tumor Resection.Clin Orthop Relat Res. 2018 Sep;476(9):1762-1770. doi: 10.1007/s11999.0000000000000165. Clin Orthop Relat Res. 2018. PMID: 30794213 Free PMC article.
References
-
- Bus MP, Szafranski A, Sellevold S, Goryn T, Jutte PC, Bramer JA, Fiocco M, Streitburger A, Kotrych D, van de Sande MA, Dijkstra PD. LUMiC® endoprosthetic reconstruction after periacetabular tumor resection: short-term results. Clin Orthop Relat Res. 2017;475:686–695. doi: 10.1007/s11999-016-4805-4. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
