

Vaginal progesterone pessaries for pregnant women with a previous preterm birth to prevent neonatal respiratory distress syndrome (the PROGRESS Study): A multicentre, randomised, placebo-controlled trial
- PMID: 28949973
- PMCID: PMC5614421
- DOI: 10.1371/journal.pmed.1002390
Vaginal progesterone pessaries for pregnant women with a previous preterm birth to prevent neonatal respiratory distress syndrome (the PROGRESS Study): A multicentre, randomised, placebo-controlled trial
Abstract
Background: Neonatal respiratory distress syndrome, as a consequence of preterm birth, is a major cause of early mortality and morbidity. The withdrawal of progesterone, either actual or functional, is thought to be an antecedent to the onset of labour. There remains limited information on clinically relevant health outcomes as to whether vaginal progesterone may be of benefit for pregnant women with a history of a previous preterm birth, who are at high risk of a recurrence. Our primary aim was to assess whether the use of vaginal progesterone pessaries in women with a history of previous spontaneous preterm birth reduced the risk and severity of respiratory distress syndrome in their infants, with secondary aims of examining the effects on other neonatal morbidities and maternal health and assessing the adverse effects of treatment.
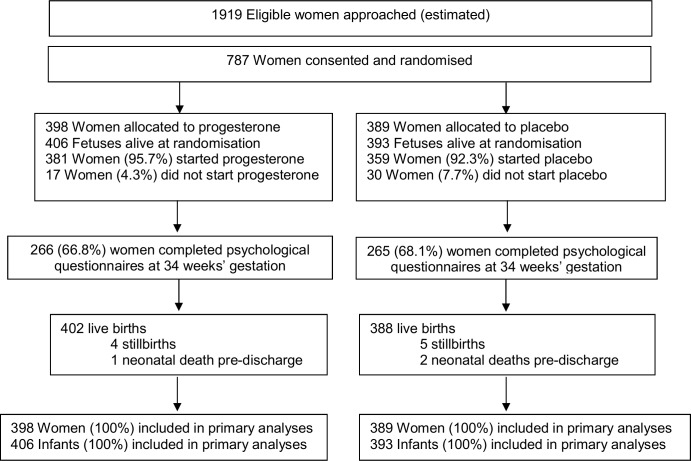
Methods: Women with a live singleton or twin pregnancy between 18 to <24 weeks' gestation and a history of prior preterm birth at less than 37 weeks' gestation in the preceding pregnancy, where labour occurred spontaneously or in association with cervical incompetence or following preterm prelabour rupture of the membranes, were eligible. Women were recruited from 39 Australian, New Zealand, and Canadian maternity hospitals and assigned by randomisation to vaginal progesterone pessaries (equivalent to 100 mg vaginal progesterone) (n = 398) or placebo (n = 389). Participants and investigators were masked to the treatment allocation. The primary outcome was respiratory distress syndrome and severity. Secondary outcomes were other respiratory morbidities; other adverse neonatal outcomes; adverse outcomes for the woman, especially related to preterm birth; and side effects of progesterone treatment. Data were analysed for all the 787 women (100%) randomised and their 799 infants.
Findings: Most women used their allocated study treatment (740 women, 94.0%), with median use similar for both study groups (51.0 days, interquartile range [IQR] 28.0-69.0, in the progesterone group versus 52.0 days, IQR 27.0-76.0, in the placebo group). The incidence of respiratory distress syndrome was similar in both study groups-10.5% (42/402) in the progesterone group and 10.6% (41/388) in the placebo group (adjusted relative risk [RR] 0.98, 95% confidence interval [CI] 0.64-1.49, p = 0.912)-as was the severity of any neonatal respiratory disease (adjusted treatment effect 1.02, 95% CI 0.69-1.53, p = 0.905). No differences were seen between study groups for other respiratory morbidities and adverse infant outcomes, including serious infant composite outcome (155/406 [38.2%] in the progesterone group and 152/393 [38.7%] in the placebo group, adjusted RR 0.98, 95% CI 0.82-1.17, p = 0.798). The proportion of infants born before 37 weeks' gestation was similar in both study groups (148/406 [36.5%] in the progesterone group and 146/393 [37.2%] in the placebo group, adjusted RR 0.97, 95% CI 0.81-1.17, p = 0.765). A similar proportion of women in both study groups had maternal morbidities, especially those related to preterm birth, or experienced side effects of treatment. In 9.9% (39/394) of the women in the progesterone group and 7.3% (28/382) of the women in the placebo group, treatment was stopped because of side effects (adjusted RR 1.35, 95% CI 0.85-2.15, p = 0.204). The main limitation of the study was that almost 9% of the women did not start the medication or forgot to use it 3 or more times a week.
Conclusions: Our results do not support the use of vaginal progesterone pessaries in women with a history of a previous spontaneous preterm birth to reduce the risk of neonatal respiratory distress syndrome or other neonatal and maternal morbidities related to preterm birth. Individual participant data meta-analysis of the relevant trials may identify specific women for whom vaginal progesterone might be of benefit.
Trial registration: Current Clinical Trials ISRCTN20269066.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: VF’s salary is part-funded through the National Health and Medical Research Council (NHMRC) of Australia. VF is also a lead investigator on a national program funded by the NHMRC to raise awareness and conduct research into stillbirth in Australia. The other authors have declared that no competing interests exist.
Figures
Comment in
-
Preterm birth prevention-Time to PROGRESS beyond progesterone.PLoS Med. 2017 Sep 26;14(9):e1002391. doi: 10.1371/journal.pmed.1002391. eCollection 2017 Sep. PLoS Med. 2017. PMID: 28949963 Free PMC article.
References
-
- March of Dimes, PMNCH, Save the Children, WHO. Born Too Soon: The Global Action Report of Preterm Birth. Eds Howsom CP, Kinney MV, Lawn JE. WHO, Geneva, 2012.
-
- Colicchia LC, Simhan HN. Optimizing subsequent pregnancy outcomes for women with a prior preterm birth. American Journal of Perinatology. 2016;33(3):267–75. doi: 10.1055/s-0035-1571143 - DOI - PubMed
-
- Gibson AM, Doyle LW. Respiratory outcomes for the tiniest or most immature infants. Seminars in Fetal & Neonatal Medicine. 2014;19(2):105–11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
