

Management of precancerous anal intraepithelial lesions in human immunodeficiency virus-positive men who have sex with men: Clinical effectiveness and cost-effectiveness
- PMID: 28950043
- PMCID: PMC5693634
- DOI: 10.1002/cncr.31035
Management of precancerous anal intraepithelial lesions in human immunodeficiency virus-positive men who have sex with men: Clinical effectiveness and cost-effectiveness
Abstract
Background: Human immunodeficiency virus (HIV)-positive men who have sex with men (MSM) are at disproportionately high risk for anal cancer. There is no definitive approach to the management of high-grade squamous intraepithelial lesions (HSIL), which are precursors of anal cancer, and evidence suggests that posttreatment adjuvant quadrivalent human papillomavirus (qHPV) vaccination improves HSIL treatment effectiveness. The objectives of this study were to evaluate the optimal HSIL management strategy with respect to clinical effectiveness and cost-effectiveness and to identify the optimal age for initiating HSIL management.
Methods: A decision analytic model of the natural history of anal carcinoma and HSIL management strategies was constructed for HIV-positive MSM who were 27 years old or older. The model was informed by the Surveillance, Epidemiology, and End Results-Medicare database and published studies. Outcomes included the lifetime cost, life expectancy, quality-adjusted life expectancy, cumulative risk of cancer and cancer-related deaths, and cost-effectiveness from a societal perspective.
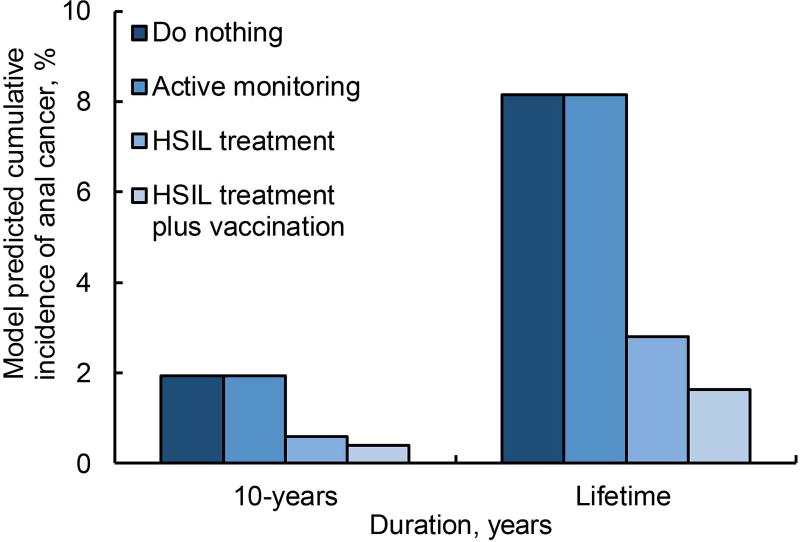
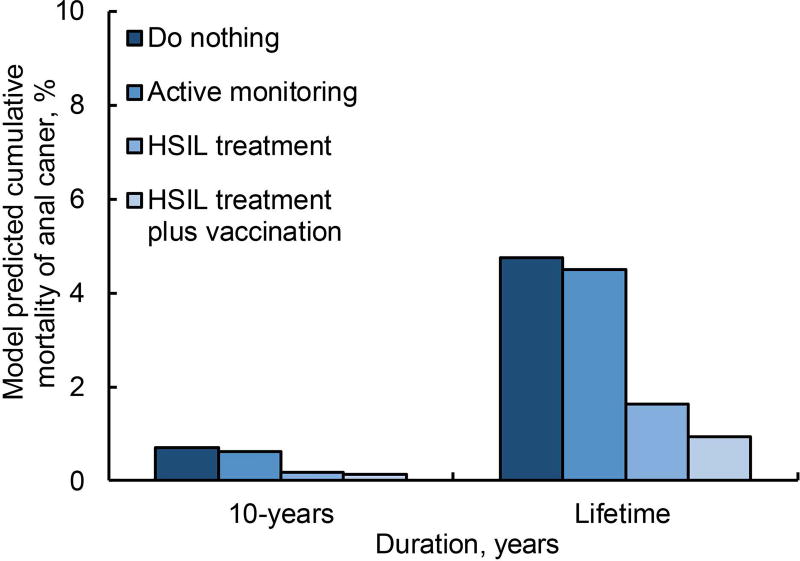
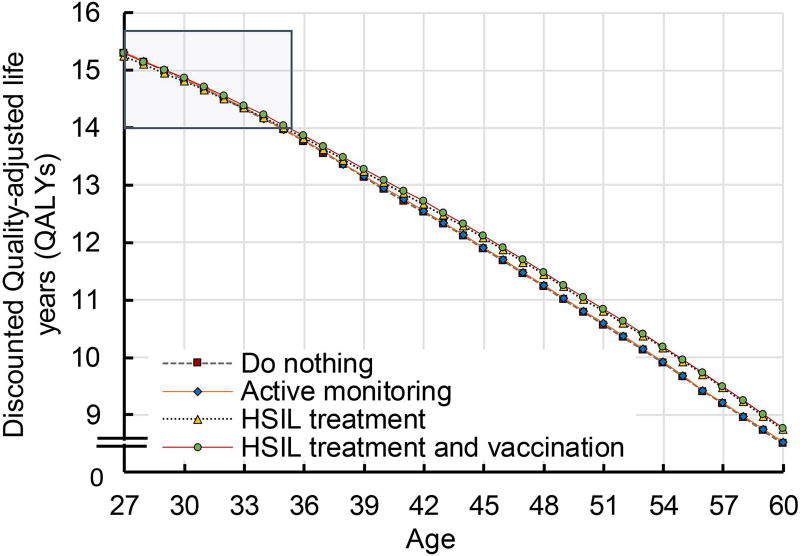
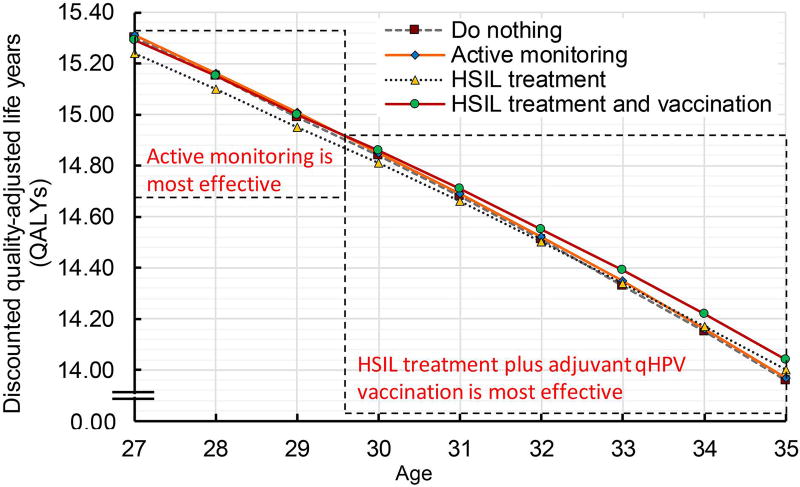
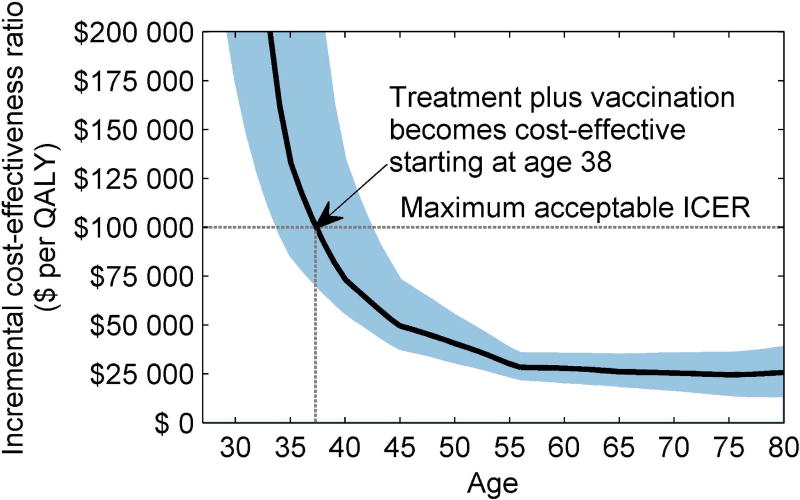
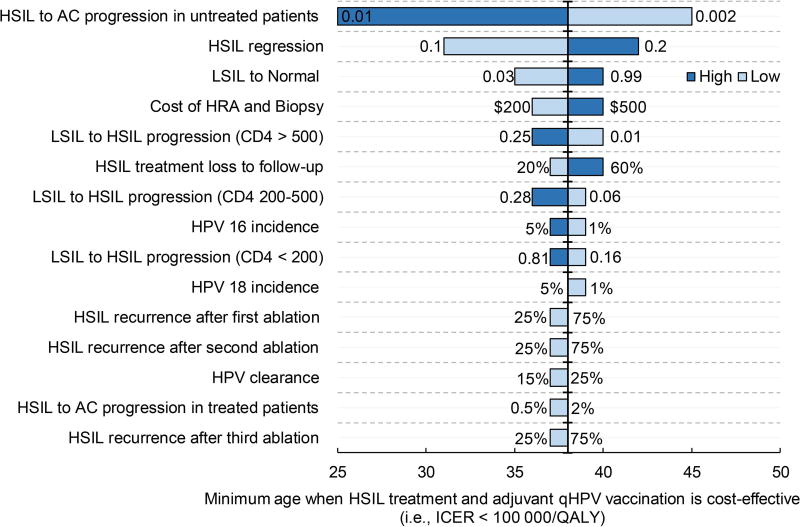
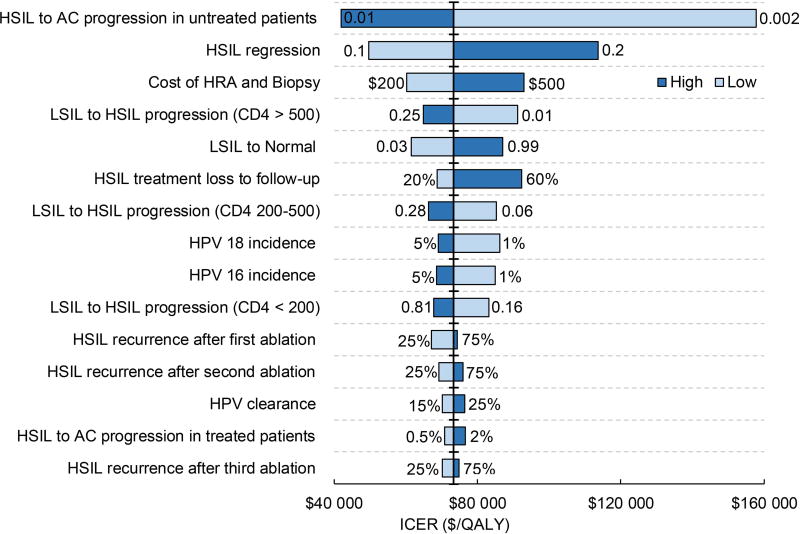
Results: Active monitoring was the most effective approach in patients 29 years or younger; thereafter, HSIL treatment plus adjuvant qHPV vaccination became most effective. When cost-effectiveness was considered (ie, an incremental cost-effectiveness ratio [ICER] < $100,000/quality-adjusted life-year), do nothing was cost-effective until the age of 38 years, and HSIL treatment plus adjuvant qHPV vaccination was cost-effective beyond the age of 38 years (95% confidence interval, 34-43 years). The ICER decreased as the age at HSIL management increased. Outcomes were sensitive to the rate of HSIL regression or progression and the cost of high-resolution anoscopy and biopsy.
Conclusions: The management of HSIL in HIV-positive MSM who are 38 years old or older with treatment plus adjuvant qHPV vaccination is likely to be cost-effective. The conservative approach of no treatment is likely to be cost-effective in younger patients. Cancer 2017;123:4709-4719. © 2017 American Cancer Society.
Keywords: anal cancer; cost-effectiveness; high-grade squamous intraepithelial lesion; human papillomavirus; human papillomavirus vaccine; management; precursor; treatment.
© 2017 American Cancer Society.
Conflict of interest statement
Figures
Comment in
-
From clinical epidemiology to practice recommendations: Knowledge gaps and uncertainty in the management of anal precancers.Cancer. 2017 Dec 1;123(23):4530-4534. doi: 10.1002/cncr.31033. Epub 2017 Sep 26. Cancer. 2017. PMID: 28949415 Free PMC article.
References
-
- Piketty C, Selinger-Leneman H, Bouvier AM, et al. Incidence of HIV-related anal cancer remains increased despite long-term combined antiretroviral treatment: results from the french hospital database on HIV. J Clin Oncol. 2012;30(35):4360–6. - PubMed
-
- Daling JR, Weiss NS, Hislop TG, et al. Sexual practices, sexually transmitted diseases, and the incidence of anal cancer. N Engl J Med. 1987;317(16):973–7. - PubMed
-
- zur Hausen H. Papillomaviruses causing cancer: evasion from host-cell control in early events in carcinogenesis. J Natl Cancer Inst. 2000;92(9):690–8. - PubMed
-
- Machalek DA, Poynten M, Jin F, et al. Anal human papillomavirus infection and associated neoplastic lesions in men who have sex with men: a systematic review and meta-analysis. Lancet Oncol. 2012;13(5):487–500. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
