

Assessment of intracranial vessels in association with carotid atherosclerosis and brain vascular lesions in rheumatoid arthritis
- PMID: 28950911
- PMCID: PMC5615800
- DOI: 10.1186/s13075-017-1422-x
Assessment of intracranial vessels in association with carotid atherosclerosis and brain vascular lesions in rheumatoid arthritis
Abstract
Background: Stroke has been associated with rheumatoid arthritis (RA). We assessed patients with RA and healthy control subjects by transcranial Doppler (TCD), carotid ultrasonography and brain magnetic resonance imaging (MRI).
Methods: Altogether, 41 female patients with RA undergoing methotrexate (MTX) or biologic treatment and 60 age-matched control subjects underwent TCD assessment of the middle cerebral artery (MCA) and basilar artery. Pulsatility index (PI), resistivity (resistance) index (RI) and circulatory reserve capacity (CRC) were determined at rest (r) and after apnoea (a) and hyperventilation (h). The presence of carotid plaques and carotid intima-media thickness (cIMT) were also determined. Intracerebral vascular lesions were investigated by brain MRI.
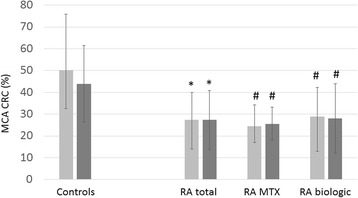
Results: MCA PI and RI values at rest and after apnoea were significantly increased in the total and MTX-treated RA populations vs control subjects. MCA CRC was also impaired, and basilar artery PI was higher in RA. More patients with RA had carotid plaques and increased cIMT. Linear regression analysis revealed that left PI(r) and RI(r) correlated with disease duration and that left PI(r), RI(r), PI(a), PI(h) and basilar PI correlated with disease activity. Right CRC inversely correlated with 28-joint Disease Activity Score. Disease activity was an independent determinant of left PI(a) and right CRC. Compared with long-term MTX treatment alone, the use of biologics in combination with MTX was associated with less impaired cerebral circulation. Impaired cerebral circulation was also associated with measures of carotid atherosclerosis.
Conclusions: To our knowledge, this is the first study to show increased distal MCA and basilar artery occlusion in RA as determined by TCD. Patients with RA also had CRC defects. We also confirmed increased carotid plaque formation and increased cIMT. Biologics may beneficially influence some parameters in the intracranial vessels.
Keywords: Biologic therapy; Carotid artery; Cerebrovascular disease; Methotrexate; Rheumatoid arthritis; Stroke; Transcranial Doppler.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval (1046-63/2015) was obtained from the Regional/Institutional Review Board of Miskolc University. The study was performed according to the principles of the Declaration of Helsinki.
Consent for publication
No data that could identify individual patients are presented; therefore, consent was not needed.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



Similar articles
-
Assessment of cognitive function in female rheumatoid arthritis patients: associations with cerebrovascular pathology, depression and anxiety.Rheumatol Int. 2020 Apr;40(4):529-540. doi: 10.1007/s00296-019-04449-8. Epub 2019 Sep 25. Rheumatol Int. 2020. PMID: 31555886
-
Effects of Methotrexate on Carotid Intima-media Thickness in Patients with Rheumatoid Arthritis.J Korean Med Sci. 2015 Nov;30(11):1589-96. doi: 10.3346/jkms.2015.30.11.1589. Epub 2015 Oct 16. J Korean Med Sci. 2015. PMID: 26539002 Free PMC article. Clinical Trial.
-
Increased thickness of the arterial intima-media detected by ultrasonography in patients with rheumatoid arthritis.Arthritis Rheum. 2002 Jun;46(6):1489-97. doi: 10.1002/art.10269. Arthritis Rheum. 2002. PMID: 12115178
-
Rheumatoid Arthritis: Atherosclerosis Imaging and Cardiovascular Risk Assessment Using Machine and Deep Learning-Based Tissue Characterization.Curr Atheroscler Rep. 2019 Jan 25;21(2):7. doi: 10.1007/s11883-019-0766-x. Curr Atheroscler Rep. 2019. PMID: 30684090 Review.
-
Recovery from rheumatoid cerebral vasculitis by low-dose methotrexate.Intern Med. 1994 Oct;33(10):615-20. doi: 10.2169/internalmedicine.33.615. Intern Med. 1994. PMID: 7827378 Review.
Cited by
-
Amelioration of gait and balance disorders by rosuvastatin is associated with changes in cerebrovascular reactivity in older patients with hypertensive treatment.Hypertens Res. 2024 Sep;47(9):2250-2261. doi: 10.1038/s41440-024-01720-9. Epub 2024 May 20. Hypertens Res. 2024. PMID: 38769134 Clinical Trial.
-
Assessment of cognitive function in female rheumatoid arthritis patients: associations with cerebrovascular pathology, depression and anxiety.Rheumatol Int. 2020 Apr;40(4):529-540. doi: 10.1007/s00296-019-04449-8. Epub 2019 Sep 25. Rheumatol Int. 2020. PMID: 31555886
-
Interdisciplinary Rheumatoid Arthritis Research and Patient Care: An Introduction and Critique of the Biopsychosocial Model of Disease Experience in Rheumatoid Arthritis.Am J Lifestyle Med. 2024 Nov 11:15598276241298937. doi: 10.1177/15598276241298937. Online ahead of print. Am J Lifestyle Med. 2024. PMID: 39540189 Free PMC article.
-
Treatment Strategies for Basilar Top Syndrome Caused by Acute Vertebral Artery Occlusion.J Neuroendovasc Ther. 2020;14(6):215-221. doi: 10.5797/jnet.cr.2019-0024. Epub 2020 Mar 31. J Neuroendovasc Ther. 2020. PMID: 37501701 Free PMC article.
-
The Microbial Metabolite Trimethylamine N-Oxide Links Vascular Dysfunctions and the Autoimmune Disease Rheumatoid Arthritis.Nutrients. 2019 Aug 7;11(8):1821. doi: 10.3390/nu11081821. Nutrients. 2019. PMID: 31394758 Free PMC article. Review.
References
-
- Sodergren A, Stegmayr B, Ohman ML, Wallberg-Jonsson S. Increased incidence of stroke and impaired prognosis after stroke among patients with seropositive rheumatoid arthritis. Clin Exp Rheumatol. 2009;27(4):641–644. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
