

Familial Liability to Epilepsy and Attention-Deficit/Hyperactivity Disorder: A Nationwide Cohort Study
- PMID: 28950988
- PMCID: PMC5723535
- DOI: 10.1016/j.biopsych.2017.08.006
Familial Liability to Epilepsy and Attention-Deficit/Hyperactivity Disorder: A Nationwide Cohort Study
Abstract
Background: Epilepsy and attention-deficit/hyperactivity disorder (ADHD) are strongly associated; however, the underlying factors contributing to their co-occurrence remain unclear. A shared genetic liability has been proposed as one possible mechanism. Therefore, our goal in this study was to investigate the familial coaggregation of epilepsy and ADHD and to estimate the contribution of genetic and environmental risk factors to their co-occurrence.
Methods: We identified 1,899,654 individuals born between 1987 and 2006 via national Swedish registers and linked each individual to his or her biological relatives. We used logistic regression to estimate the association between epilepsy and ADHD within individual and across relatives. Quantitative genetic modeling was used to decompose the cross-disorder covariance into genetic and environmental factors.
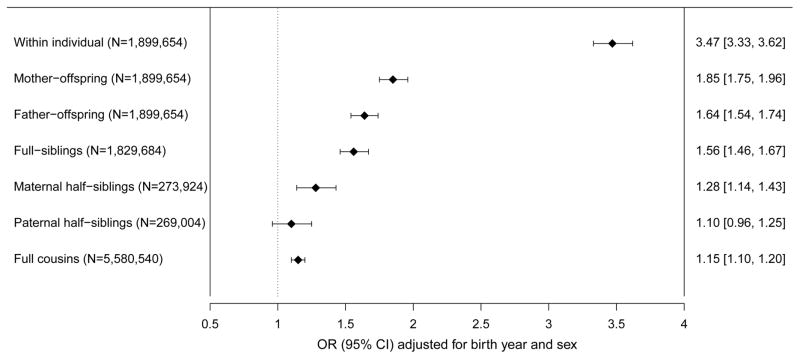
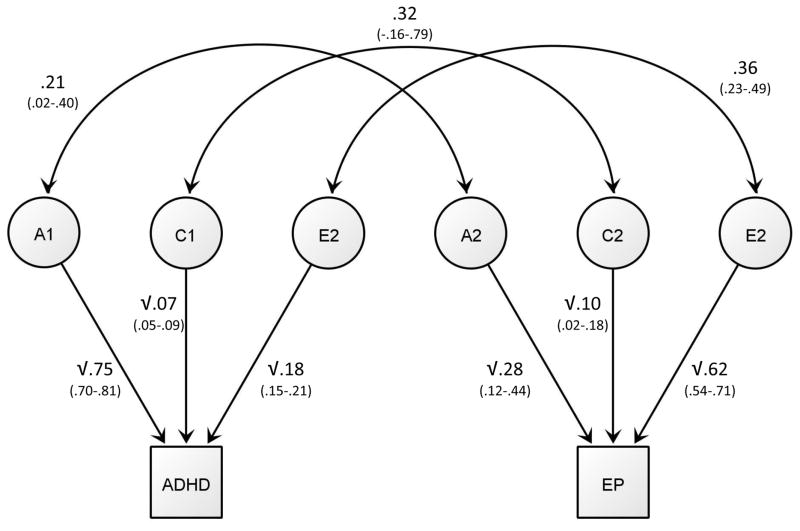
Results: Individuals with epilepsy had a statistically significant increased risk of ADHD (odds ratio [OR] = 3.47, 95% confidence interval [CI] = 3.33-3.62). This risk increase extended to children whose mothers had epilepsy (OR = 1.85, 95% CI = 1.75-1.96), children whose fathers had epilepsy (OR = 1.64, 95% CI = 1.54-1.74), full siblings (OR = 1.56, 95% CI = 1.46-1.67), maternal half siblings (OR = 1.28, 95% CI = 1.14-1.43), paternal half siblings (OR = 1.10, 95% CI = 0.96-1.25), and cousins (OR = 1.15, 95% CI = 1.10-1.20). The genetic correlation was 0.21 (95% CI = 0.02-0.40) and explained 40% of the phenotypic correlation between epilepsy and ADHD, with the remaining variance largely explained by nonshared environmental factors (49%, nonshared environmental correlation = 0.36, 95% CI = 0.23-0.49). The contribution of shared environmental factors to the cross-disorder overlap was not statistically significant (11%, shared environmental correlation = 0.32, 95% CI = -0.16-0.79).
Conclusions: This study demonstrates a strong and etiologically complex association between epilepsy and ADHD, with shared familial factors and risk factors unique to the individual contributing to co-occurrence of the disorders. Our findings suggest that epilepsy and ADHD may share less genetic risk as compared with other neurodevelopmental disorders.
Keywords: ADHD; Comorbidity; Epilepsy; Genetics; Neurodevelopment; Risk factors.
Copyright © 2017 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Links Between Epilepsy and ADHD: Time to Focus and Act.Epilepsy Curr. 2018 May-Jun;18(3):160-161. doi: 10.5698/1535-7597.18.3.160. Epilepsy Curr. 2018. PMID: 29950937 Free PMC article. No abstract available.
References
-
- Russ SA, Larson K, Halfon N. A national profile of childhood epilepsy and seizure disorder. Pediatrics. 2012;129:256–264. - PubMed
-
- Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. 2015;56:345–365. - PubMed
-
- Aaberg KM, Bakken IJ, Lossius MI, Lund Soraas C, Haberg SE, Stoltenberg C, et al. Comorbidity and Childhood Epilepsy: A Nationwide Registry Study. Pediatrics. 2016:138. - PubMed
-
- Bertelsen EN, Larsen JT, Petersen L, Christensen J, Dalsgaard S. Childhood Epilepsy, Febrile Seizures, and Subsequent Risk of ADHD. Pediatrics. 2016:138. - PubMed
-
- Hamoda HM, Guild DJ, Gumlak S, Travers BH, Gonzalez-Heydrich J. Association between attention-deficit/hyperactivity disorder and epilepsy in pediatric populations. Expert Rev Neurother. 2009;9:1747–1754. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
