

Prophylactic negative-pressure wound therapy after cesarean is associated with reduced risk of surgical site infection: a systematic review and meta-analysis
- PMID: 28951263
- PMCID: PMC5807120
- DOI: 10.1016/j.ajog.2017.09.017
Prophylactic negative-pressure wound therapy after cesarean is associated with reduced risk of surgical site infection: a systematic review and meta-analysis
Abstract
Objective: The objective of the study was to assess the effect of prophylactic negative-pressure wound therapy on surgical site infections and other wound complications in women after cesarean delivery.
Data sources: We searched Ovid Medline, Embase, SCOPUS, Cochrane Database of Systematic Reviews, and ClinicalTrials.gov.
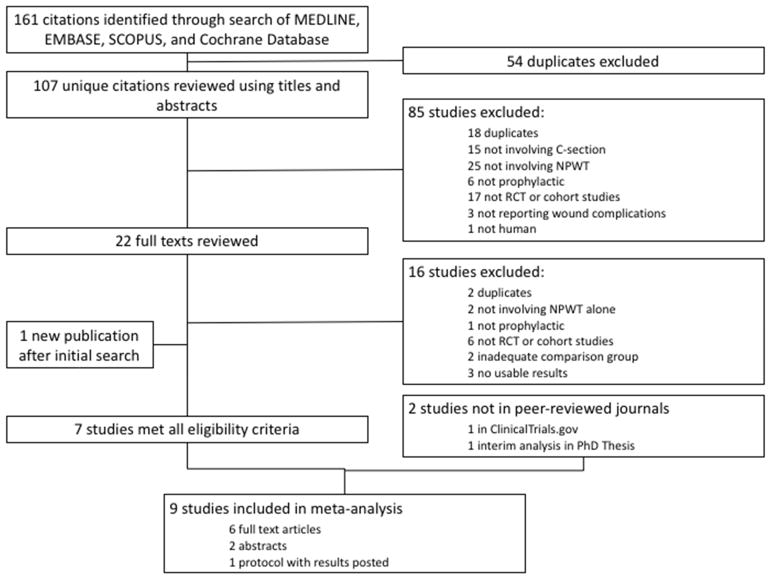
Study eligibility criteria: We included randomized controlled trials and observational studies comparing prophylactic negative-pressure wound therapy with standard wound dressing for cesarean delivery.
Study appraisal and synthesis methods: The primary outcome was surgical site infection after cesarean delivery. Secondary outcomes were composite wound complications, wound dehiscence, wound seroma, endometritis, and hospital readmission. Heterogeneity was assessed using Higgin's I2. Relative risks with 95% confidence intervals were calculated using random-effects models.
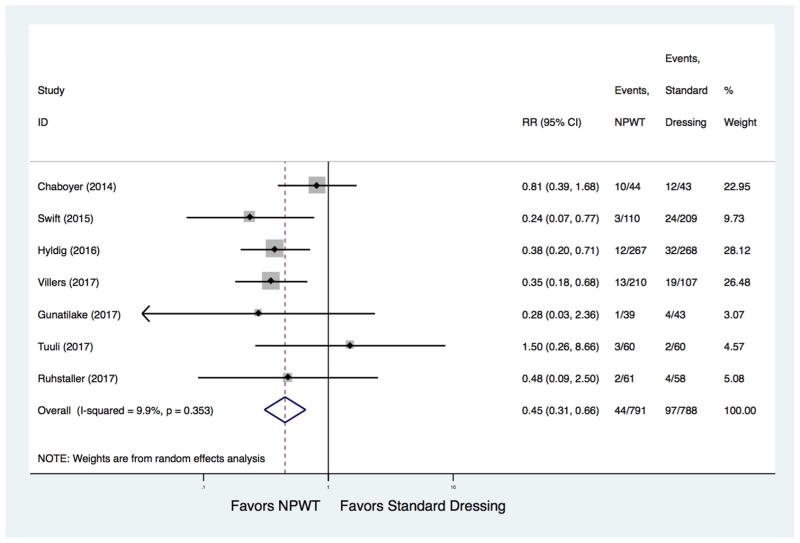
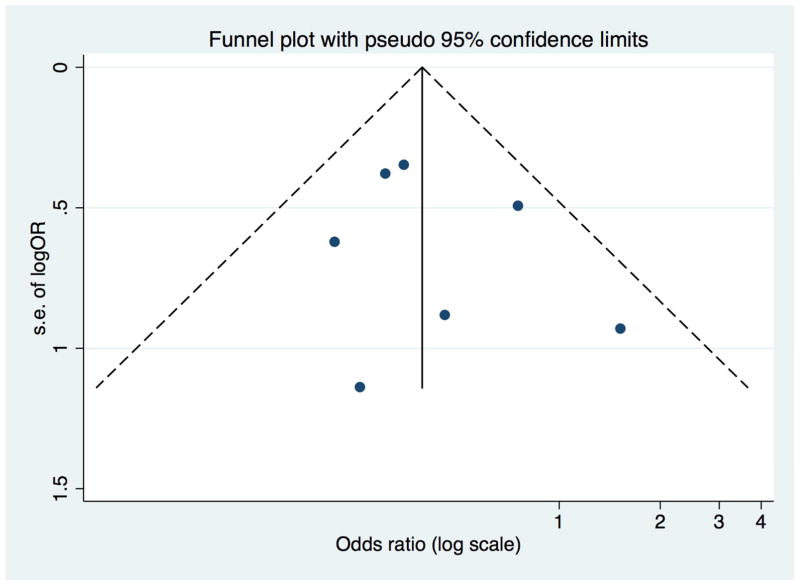
Results: Six randomized controlled trials and 3 cohort studies in high-risk mostly obese women met inclusion criteria and were included in the meta-analysis. Six were full-text articles, 2 published abstracts, and 1 report of trial results in ClinicalTrials.gov. Studies were also heterogeneous in the patients included and type of negative-pressure wound therapy device. The risk of surgical site infection was significantly lower with the use of prophylactic negative-pressure wound therapy compared with standard wound dressing (7 studies: pooled risk ratio, 0.45; 95% confidence interval, 0.31-0.66; adjusted risk ratio, -6.0%, 95% confidence interval, -10.0% to -3.0%; number needed to treat, 17, 95% confidence interval, 10-34). There was no evidence of significant statistical heterogeneity (I2 = 9.9%) or publication bias (Egger P = .532). Of the secondary outcomes, only composite wound complications were significantly reduced in patients receiving prophylactic negative-pressure wound therapy compared with standard dressing (9 studies: pooled risk ratio, 0.68, 95% confidence interval, 0.49-0.94).
Conclusion: Studies on the effectiveness of prophylactic negative-pressure wound therapy at cesarean delivery are heterogeneous but suggest a reduction in surgical site infection and overall wound complications. Larger definitive trials are needed to clarify the clinical utility of prophylactic negative-pressure wound therapy after cesarean delivery.
Keywords: antibiotics; cesarean delivery; dehiscence; endometritis; hospital readmission; meta-analysis; prophylactic negative-pressure wound therapy; seroma; surgical site infection.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Apparently conflicting meta-analyses on prophylactic negative pressure wound therapy after cesarean delivery.Am J Obstet Gynecol. 2018 Sep;219(3):311-312. doi: 10.1016/j.ajog.2018.04.034. Epub 2018 Apr 26. Am J Obstet Gynecol. 2018. PMID: 29705194 No abstract available.
References
-
- Martin JA, Hamilton BE, Osterman MJK. Births in the United States, 2015. Natl Cent Heal Stat Data Br. 2016;2015(258):1–8. http://www.ncbi.nlm.nih.gov/pubmed/27648876. - PubMed
-
- Osterman MJK, Martin JA. Trends in low-risk cesarean delivery in the United States, 1990–2013. Natl Vital Stat Reports. 2014;63(6):1–16. - PubMed
-
- Newlin C, Kuehl TJ, Pickrel A, Cawyer CR, Jones RO. Cesarean section incision complications and associated risk factors: A quality assurance project. Open J Obstet Gynecol. 2015;(November):789–794.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
