

Longitudinal Cell-Free DNA Analysis in Patients with Small Cell Lung Cancer Reveals Dynamic Insights into Treatment Efficacy and Disease Relapse
- PMID: 28951314
- PMCID: PMC5827950
- DOI: 10.1016/j.jtho.2017.09.1951
Longitudinal Cell-Free DNA Analysis in Patients with Small Cell Lung Cancer Reveals Dynamic Insights into Treatment Efficacy and Disease Relapse
Abstract
Introduction: Patients with SCLC have a poor prognosis and limited treatment options. Because access to longitudinal tumor samples is very limited in patients with this disease, we chose to focus our studies on the characterization of plasma cell-free DNA (cfDNA) for rapid, noninvasive monitoring of disease burden.
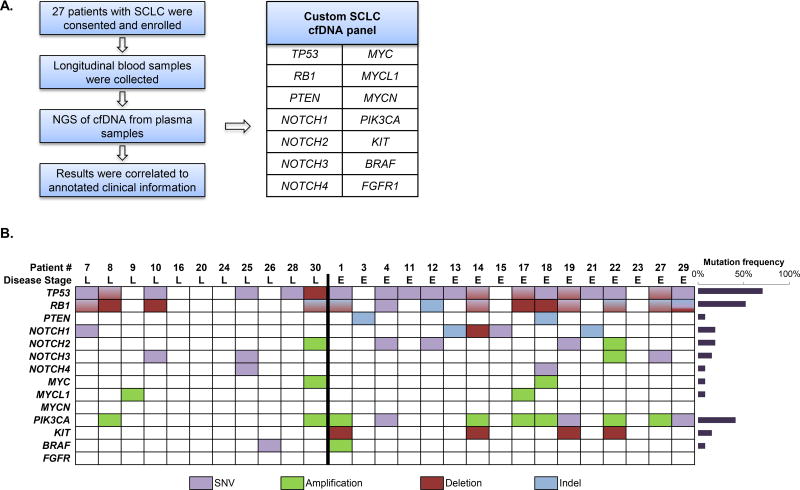
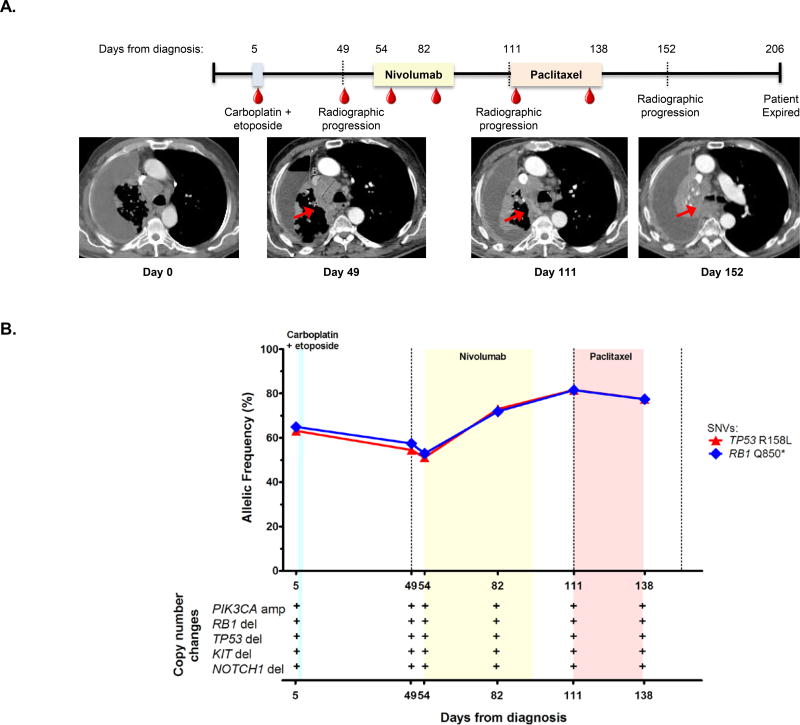
Methods: We developed a liquid biopsy assay that quantifies somatic variants in cfDNA. The assay detects single nucleotide variants, copy number alterations, and insertions or deletions in 14 genes that are frequently mutated in SCLC, including tumor protein p53 gene (TP53), retinoblastoma 1 gene (RB1), BRAF, KIT proto-oncogene receptor tyrosine kinase gene (KIT), notch 1 gene (NOTCH1), notch 2 gene (NOTCH2), notch 3 gene (NOTCH3), notch 4 gene (NOTCH4), phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha gene (PIK3CA), phosphatase and tensin homolog gene (PTEN), fibroblast growth factor receptor 1 gene (FGFR1), v-myc avian myelocytomatosis viral oncogene homolog gene (MYC), v-myc avian myelocytomatosis viral oncogene lung carcinoma derived homolog gene (MYCL1), and v-myc avian myelocytomatosis viral oncogene neuroblastoma derived homolog gene (MYCN).
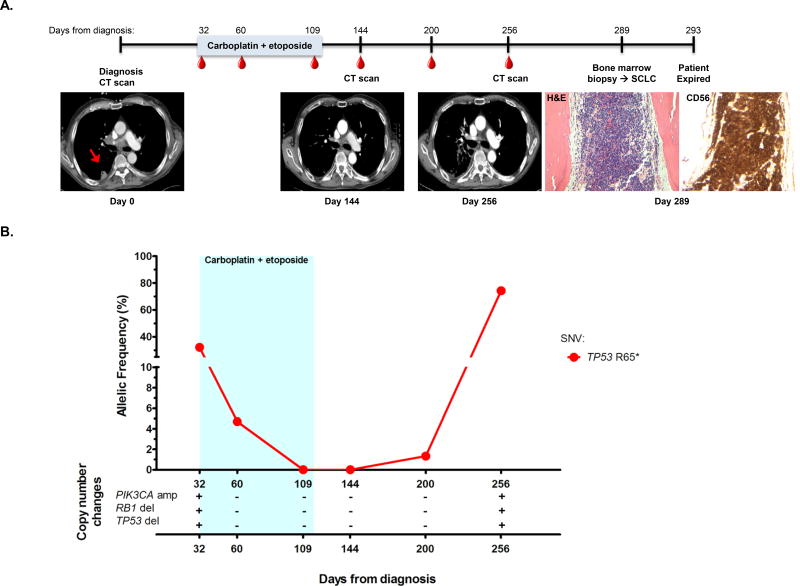
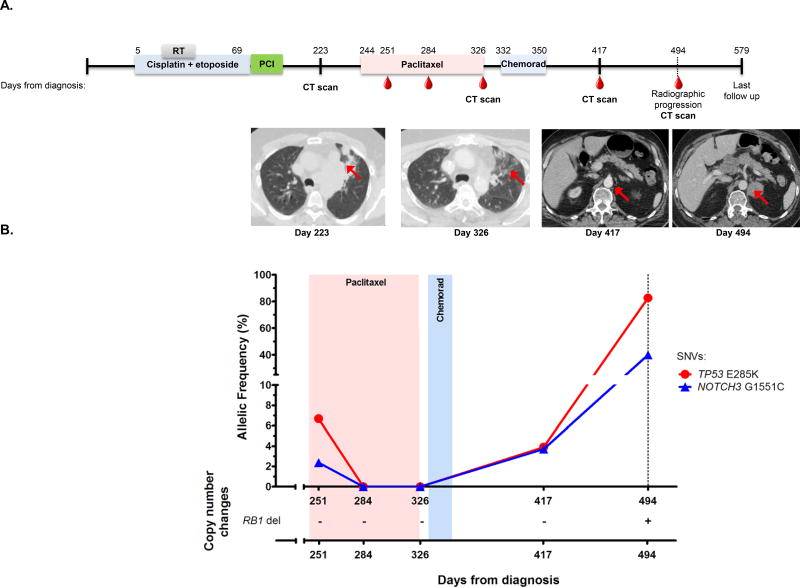
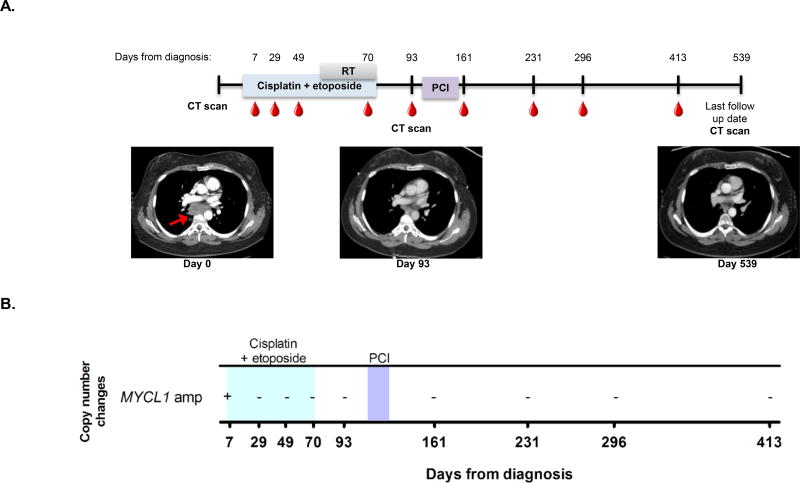
Results: Over the course of 26 months of peripheral blood collection, we examined 140 plasma samples from 27 patients. We detected disease-associated mutations in 85% of patient samples with mutant allele frequencies ranging from 0.1% to 87%. In our cohort, 59% of the patients had extensive-stage disease, and the most common mutations occurred in TP53 (70%) and RB1 (52%). In addition to mutations in TP53 and RB1, we detected alterations in 10 additional genes in our patient population (PTEN, NOTCH1, NOTCH2, NOTCH3, NOTCH4, MYC, MYCL1, PIK3CA, KIT, and BRAF). The observed allele frequencies and copy number alterations tracked closely with treatment responses. Notably, in several cases analysis of cfDNA provided evidence of disease relapse before conventional imaging.
Conclusions: These results suggest that liquid biopsies are readily applicable in patients with SCLC and can potentially provide improved monitoring of disease burden, depth of response to treatment, and timely warning of disease relapse in patients with this disease.
Keywords: Cell-free tumor DNA; Liquid biopsy; Next-generation sequencing; Plasma; Small cell lung cancer.
Copyright © 2017 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Editorial for "Longitudinal cell-free DNA analysis in patients with small cell lung cancer reveals dynamic insights into treatment efficacy and disease relapse".Transl Lung Cancer Res. 2018 Dec;7(Suppl 4):S367-S369. doi: 10.21037/tlcr.2018.09.19. Transl Lung Cancer Res. 2018. PMID: 30705858 Free PMC article. No abstract available.
References
-
- Torre LA, Siegel RL, Jemal A. Lung Cancer Statistics. Adv Exp Med Biol. 2016;893:1–19. - PubMed
-
- Bernhardt EB, Jalal SI. Small Cell Lung Cancer. Cancer Treat Res. 2016;170:301–322. - PubMed
-
- Ramalingam SS. Small-Cell Lung Cancer: New Directions for Systemic Therapy. J Oncol Pract. 2016;12(2):119–120. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
