

Magnetic Resonance Lymphangiography and Lymphatic Embolization in the Treatment of Pulmonary Complication of Lymphatic Malformation
- PMID: 28955119
- PMCID: PMC5615381
- DOI: 10.1055/s-0037-1604301
Magnetic Resonance Lymphangiography and Lymphatic Embolization in the Treatment of Pulmonary Complication of Lymphatic Malformation
Abstract
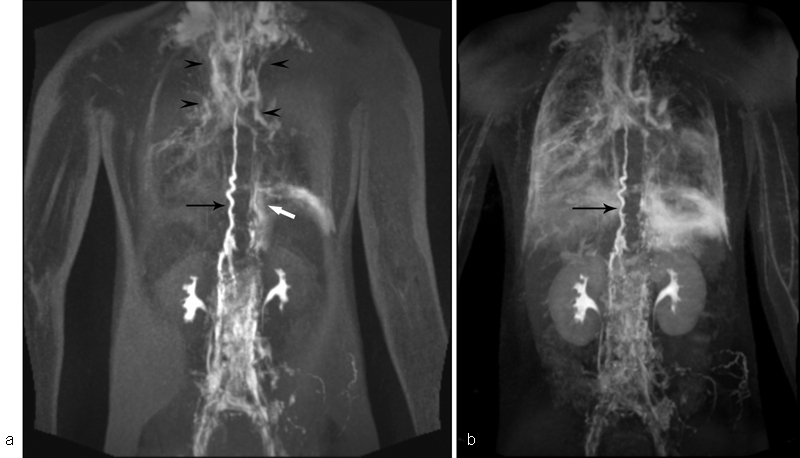
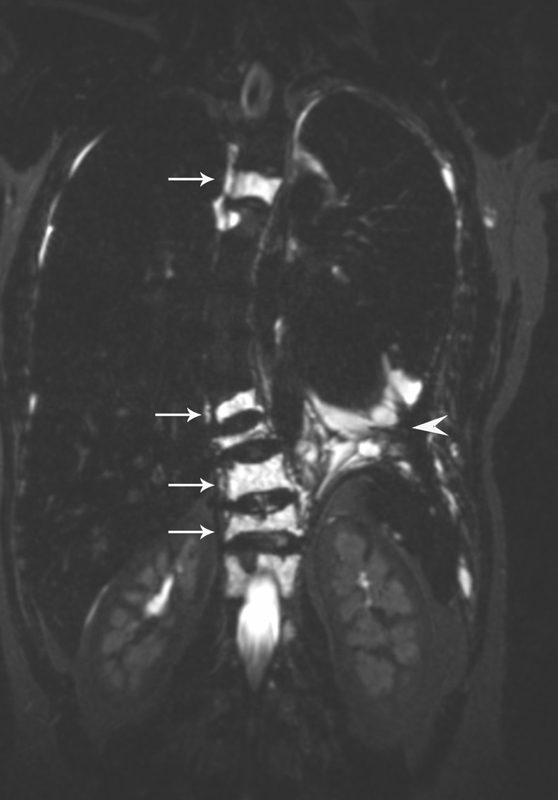
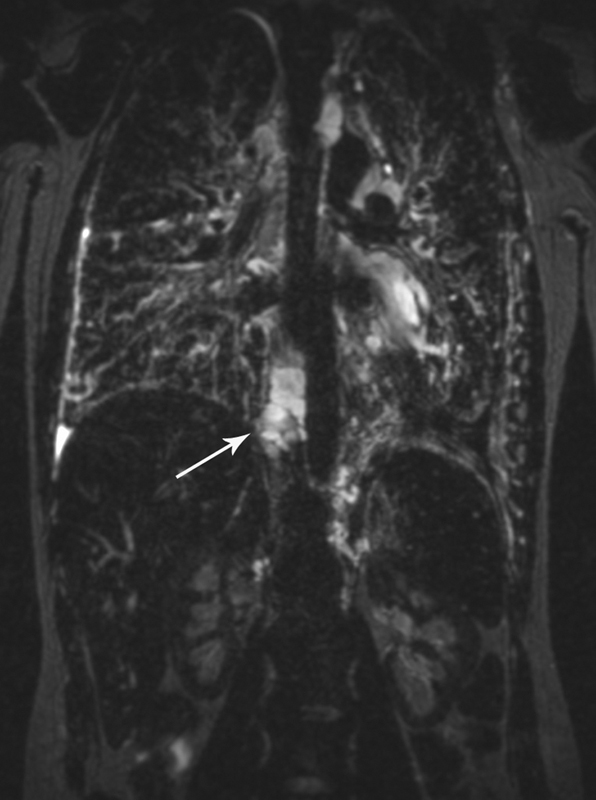
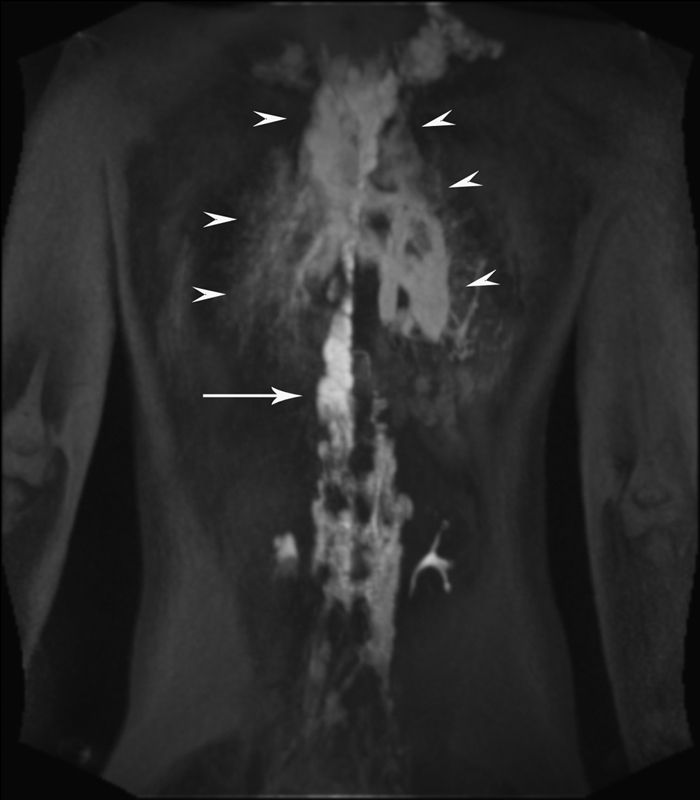
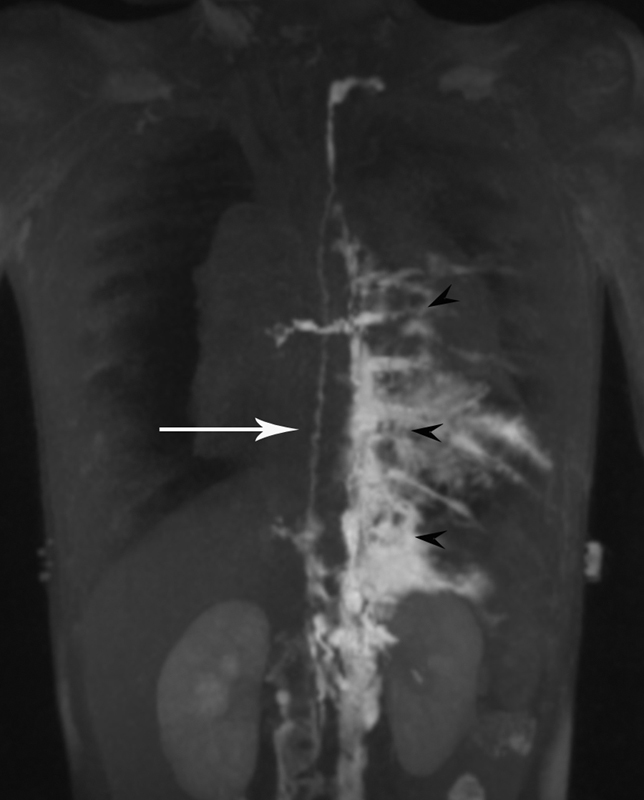
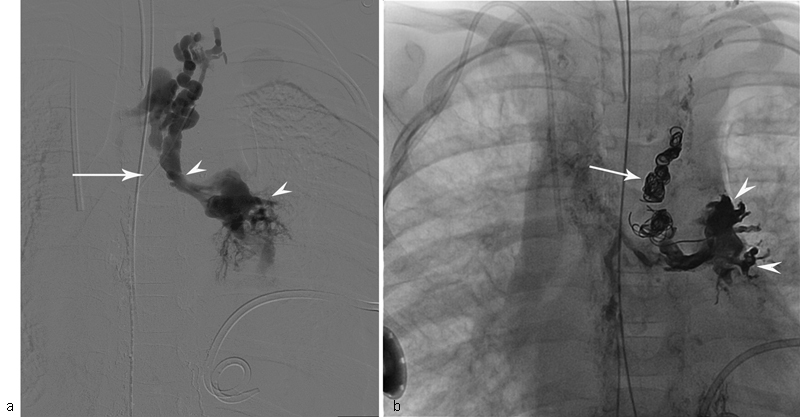
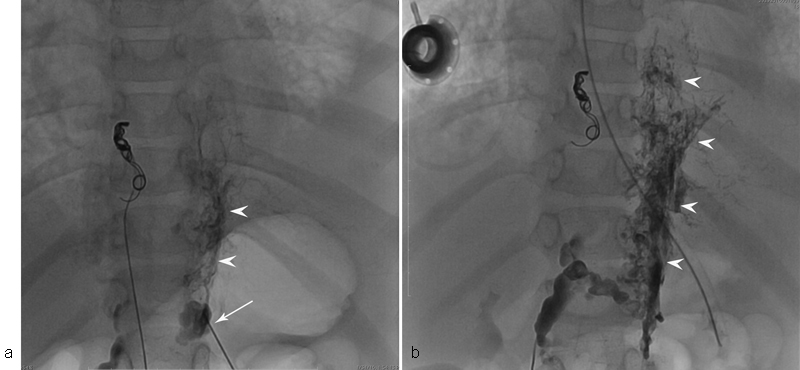
Lymphatic malformations (LMs; especially those involving the central conducting lymphatic channels) are characterized by dysplastic and incompetent lymphatic channels in multiple tissues and organs. The major cause of mortality and morbidity in patients with thoracic LM is deterioration of pulmonary function due to chronic chylous effusions and progressive interstitial lung disease. The etiology of these pulmonary processes is unknown, although lymphatic involvement is certain. Understanding of the changes in the lymphatic anatomy in patients with LM has been hindered by difficulty of imaging of the lymphatic system. Recently developed dynamic contrast-enhanced magnetic resonance lymphangiography (DCMRL) allows dynamic MR imaging of the lymphatic system by injecting gadolinium contrast agent in the groin lymph nodes. Using this technique, pathological lymphatic flow from the central lymphatic system and/or retroperitoneal and mediastinal masses into lung parenchyma ("pulmonary lymphatic perfusion syndrome") has been demonstrated in patients with LM. This abnormal lymphatic perfusion overflows pulmonary parenchyma and results in deterioration of pulmonary function due to interstitial process and/or compression effect of chylous effusions. Percutaneous thoracic duct embolization or lymphatic interstitial embolization of the lymphatic masses results in cessation of the pulmonary lymphatic overflow and significant improvement in pulmonary symptoms in these patients.
Keywords: embolization; interventional radiology; lymphangiography; lymphatic malformations; pulmonary function.
Figures
References
-
- Wassef M, Blei F, Adams D et al.Vascular anomalies classification: recommendations from the International Society for the Study of Vascular Anomalies. Pediatrics. 2015;136(01):e203–e214. - PubMed
-
- Faul J L, Berry G J, Colby T Vet al.Thoracic lymphangiomas, lymphangiectasis, lymphangiomatosis, and lymphatic dysplasia syndrome Am J Respir Crit Care Med 2000161(3, Pt 1):1037–1046. - PubMed
-
- Mitsumori L M, McDonald E S, Wilson G J, Neligan P C, Minoshima S, Maki J H. MR lymphangiography: how I do it. J Magn Reson Imaging. 2015;42(06):1465–1477. - PubMed
-
- Nadolski G J, Itkin M. Feasibility of ultrasound-guided intranodal lymphangiogram for thoracic duct embolization. J Vasc Interv Radiol. 2012;23(05):613–616. - PubMed
-
- Kerlan R K, Jr, Laberge J M. Intranodal lymphangiography: coming soon to a hospital near you. J Vasc Interv Radiol. 2012;23(05):617. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
