

Effect of Adjunct Balloon Dilation after Long Everolimus-eluting Stent Deployment on Major Adverse Cardiac Events
- PMID: 28955388
- PMCID: PMC5614946
- DOI: 10.4070/kcj.2017.0016
Effect of Adjunct Balloon Dilation after Long Everolimus-eluting Stent Deployment on Major Adverse Cardiac Events
Abstract
Background and objectives: The effectiveness of adjunct balloon dilation after drug-eluting stent (DES) deployment has not been sufficiently evaluated. We evaluated whether adjunct balloon dilation was associated with a reduction in major adverse cardiac events (MACEs) after long everolimus-eluting stents (EESs) implantation.
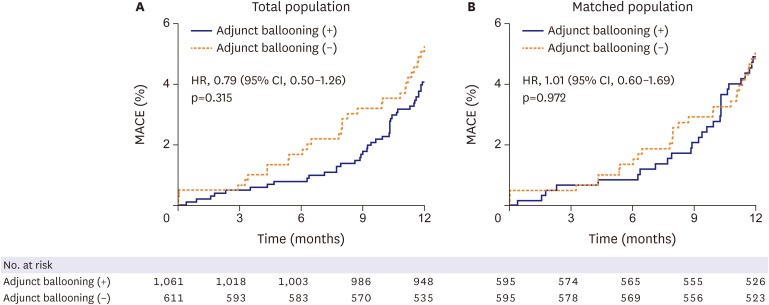
Subjects and methods: Drawing from 2 randomized trials, a total of 1,672 patients treated with long EES were analyzed. Of 1,672 patients, 1,061 patients (64%) received post-stent adjunct balloon dilation. MACE, defined as a composite of cardiac death, myocardial infarction, and target-lesion revascularization (TLR), was compared between patients who received post-stent adjunct balloon dilation and patients who did not in 595 propensity score-matched pairs.
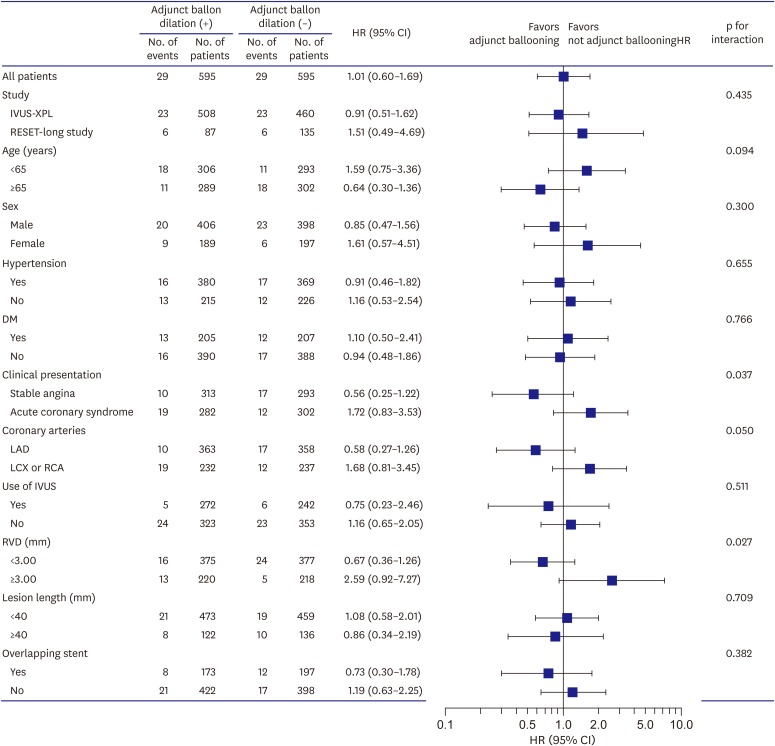
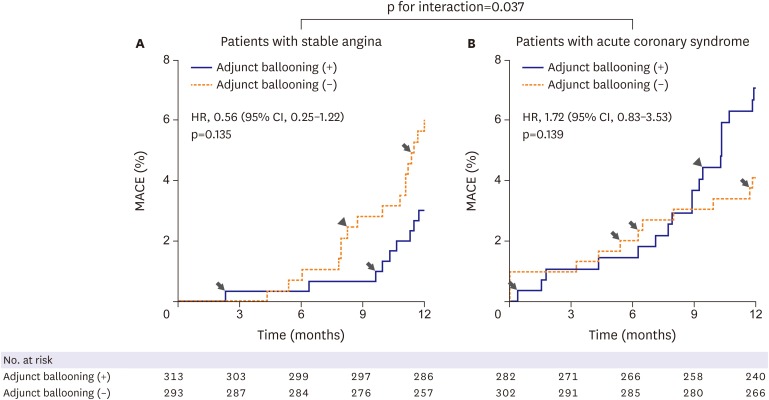
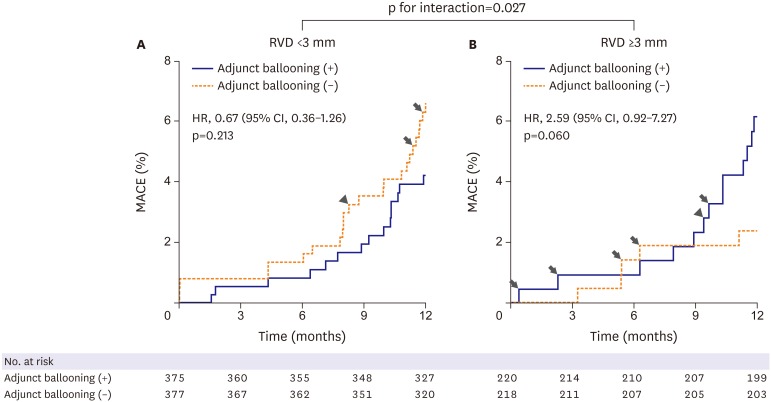
Results: For the matched population, MACE occurred in 29 patients (4.9%) who received adjunct balloon dilation and in 29 patients (4.9%) who did not (hazard ratio [HR], 1.01; 95% confidence interval [CI], 0.60-1.69; p=0.972). However, significant interactions were observed among the subgroups for clinical presentation and vessel size. Adjunct balloon dilation was more favored within the subset of patients with stable angina vs. the subset of patients with acute coronary syndrome (p for interaction=0.037), and within the subset of lesions with small vessel diameter (reference vessel diameter [RVD] <3 mm) vs. the subset of lesions with larger vessel diameter (RVD ≥3 mm; p for interaction=0.027).
Conclusion: Adjunct balloon dilation was not associated with MACE reduction at 1 year among patients requiring long EES implantation. However, post-stent adjunct balloon dilation may be necessary for patients requiring long EES implantation who present with stable angina or for lesions with small vessel diameters.
Keywords: Coronary artery disease; Drug-eluting stents; Treatment outcome.
Conflict of interest statement
Conflict of Interest: The authors have no financial conflicts of interest.
Figures
Similar articles
-
Meta-analysis of everolimus-eluting versus paclitaxel-eluting stents in coronary artery disease: final 3-year results of the SPIRIT clinical trials program (Clinical Evaluation of the Xience V Everolimus Eluting Coronary Stent System in the Treatment of Patients With De Novo Native Coronary Artery Lesions).JACC Cardiovasc Interv. 2013 Sep;6(9):914-22. doi: 10.1016/j.jcin.2013.05.005. JACC Cardiovasc Interv. 2013. PMID: 24050859
-
Randomized comparison of everolimus-eluting stents and sirolimus-eluting stents in patients with ST elevation myocardial infarction: RACES-MI trial.JACC Cardiovasc Interv. 2014 Aug;7(8):849-56. doi: 10.1016/j.jcin.2014.02.016. JACC Cardiovasc Interv. 2014. PMID: 25147029 Clinical Trial.
-
Efficacy of everolimus-eluting stent implantation in patients with small coronary arteries (≤2.5 mm): outcomes of 3-year clinical follow-up.Heart Vessels. 2017 Jul;32(7):796-803. doi: 10.1007/s00380-016-0937-4. Epub 2016 Dec 26. Heart Vessels. 2017. PMID: 28025695
-
A propensity score matched comparative study between paclitaxel-coated balloon and everolimus-eluting stents for the treatment of small coronary vessels.Catheter Cardiovasc Interv. 2017 Sep 1;90(3):380-386. doi: 10.1002/ccd.26929. Epub 2017 Jan 21. Catheter Cardiovasc Interv. 2017. PMID: 28109036
-
Efficacy and safety of everolimus and zotarolimus-eluting stents versus first-generation drug-eluting stents in patients with diabetes: A meta-analysis of randomized trials.Int J Cardiol. 2017 Mar 1;230:310-318. doi: 10.1016/j.ijcard.2016.12.116. Epub 2016 Dec 27. Int J Cardiol. 2017. PMID: 28062139 Review.
Cited by
-
Stent Optimization Using Adjunctive Balloon Dilatation in the Era of Second-Generation Drug-Eluting Stents.Korean Circ J. 2017 Sep;47(5):686-688. doi: 10.4070/kcj.2017.0160. Epub 2017 Sep 11. Korean Circ J. 2017. PMID: 28955385 Free PMC article. No abstract available.
-
The Clinical and Angiographic Outcomes of Postdilation after Percutaneous Coronary Intervention in Patients with Acute Coronary Syndrome: A Systematic Review and Meta-Analysis.J Interv Cardiol. 2021 Apr 9;2021:6699812. doi: 10.1155/2021/6699812. eCollection 2021. J Interv Cardiol. 2021. PMID: 33935601 Free PMC article.
-
Stent expansion evaluated by optical coherence tomography and subsequent outcomes.Sci Rep. 2023 Mar 7;13(1):3781. doi: 10.1038/s41598-023-30717-6. Sci Rep. 2023. PMID: 36882449 Free PMC article.
-
Performing percutaneous coronary interventions with predilatation using non-compliant balloons at high-pressure versus conventional semi-compliant balloons: insights from two randomised studies using optical coherence tomography.Open Heart. 2020 Jan 23;7(1):e001204. doi: 10.1136/openhrt-2019-001204. eCollection 2020. Open Heart. 2020. PMID: 32076567 Free PMC article.
References
-
- Brodie BR, Cooper C, Jones M, Fitzgerald P, Cummins F, Postdilatation Clinical Compartative Study (POSTIT) Investigators Is adjunctive balloon postdilatation necessary after coronary stent deployment? Final results from the POSTIT trial. Catheter Cardiovasc Interv. 2003;59:184–192. - PubMed
-
- Russo RJ, Silva PD, Teirstein PS, et al. A randomized controlled trial of angiography versus intravascular ultrasound-directed bare-metal coronary stent placement (the AVID Trial) Circ Cardiovasc Interv. 2009;2:113–123. - PubMed
-
- Hur SH, Kitamura K, Morino Y, et al. Efficacy of postdeployment balloon dilatation for current generation stents as assessed by intravascular ultrasound. Am J Cardiol. 2001;88:1114–1119. - PubMed
-
- Romagnoli E, Sangiorgi GM, Cosgrave J, Guillet E, Colombo A. Drug-eluting stenting: the case for post-dilation. JACC Cardiovasc Interv. 2008;1:22–31. - PubMed
-
- Hoffmann R, Guagliumi G, Musumeci G, et al. Vascular response to sirolimus-eluting stents delivered with a nonaggressive implantation technique: comparison of intravascular ultrasound results from the multicenter, randomized E-SIRIUS, and SIRIUS trials. Catheter Cardiovasc Interv. 2005;66:499–506. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
