

Cervical cancer in southern Malawi: A prospective analysis of presentation, management, and outcomes
- PMID: 28955419
- PMCID: PMC5610282
- DOI: 10.4314/mmj.v29i2.9
Cervical cancer in southern Malawi: A prospective analysis of presentation, management, and outcomes
Abstract
Background: Malawi has the highest age standardised rate of cervical cancer in the world. This study describes the presentation, management and short-term outcomes of patients with newly diagnosed cervical cancer at Queen Elizabeth Central Hospital (QECH), in Southern Malawi.
Methods: All patients with a new diagnosis of cervical cancer presenting to QECH between 1st January-1st July 2015 had demographic data, referral pathway, stage, histology and management prospectively recorded at presentation, and at two months after initial presentation.
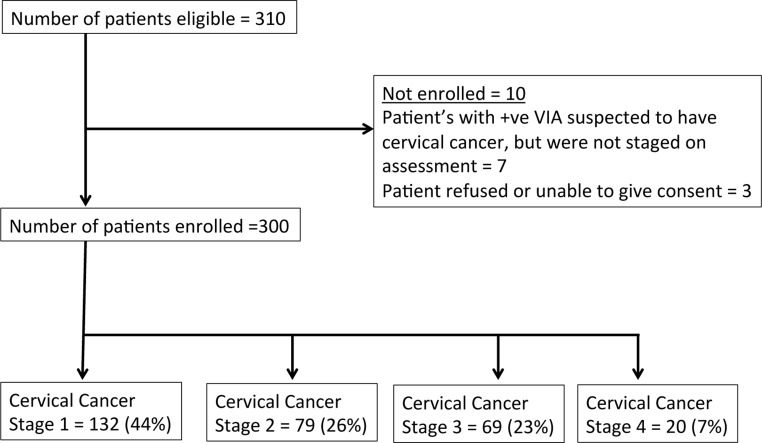
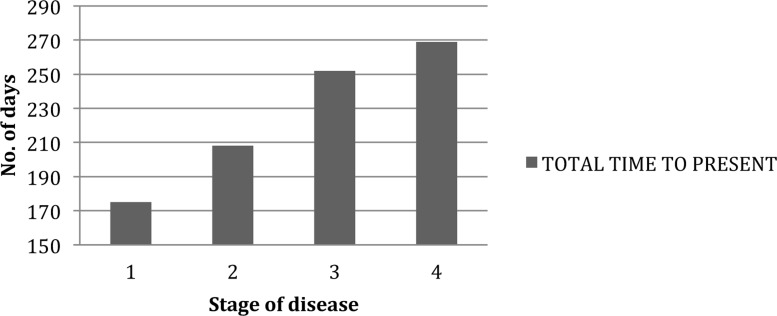
Results: 310 women presented with cervical cancer to QECH and 300 were included (mean age 44.9 years; HIV 47%), representing 8% of the estimated annual number of new presentations in Malawi. Mean age of patients with HIV was 6.9 years younger compared to those without HIV (p<0.05). 132 (44%) patients had stage 1 cervical cancer and 168 (56%) presented with more advanced disease (stage II-IV). There was a mean delay of 23.1 weeks between onset of symptoms and being seen by a clinician and a further 19 weeks before attending QECH. Most common management plans at initial consultation were: same day biopsy (n=112, 37.3%);, booking for curative surgery (n=76, 25.3%);, and referral to palliative care (n=93, 31%). At 2 months, 64 (57%) biopsies were reported, 31 (40.8%) operations were completed and 27 (29%) patients had attended the palliative clinic.
Conclusions: Patients presenting with cervical cancer to QECH were young, with a high prevalence of HIV, and late stage disease. The lack of pathological and surgical capacity and the absence of radiotherapy severely limited the possibility of curative treatment. Access to quality palliative care remains an important component of management in low resource settings. Improving awareness of cervical cancer in the community, and better recognition and management within the health service, are important in reducing the cancer burden for women in Malawi.
Figures
References
-
- Ferlay J SI, Ervik M, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11. Lyon, France: International Agency for Research on Cancer; 2013.
-
- Gondos A, et al. Cancer survival in a southern African urban population. Int J Cancer. 2004;112(5):860–864. - PubMed