

The Medina Embolic Device: Karolinska experience
- PMID: 28956513
- PMCID: PMC5772534
- DOI: 10.1177/1591019917733125
The Medina Embolic Device: Karolinska experience
Abstract
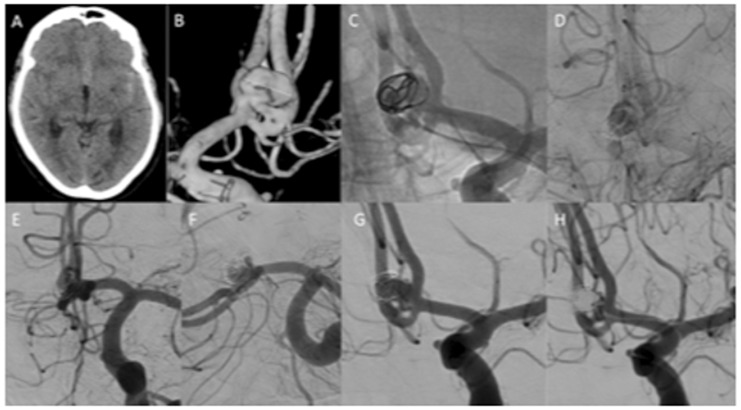
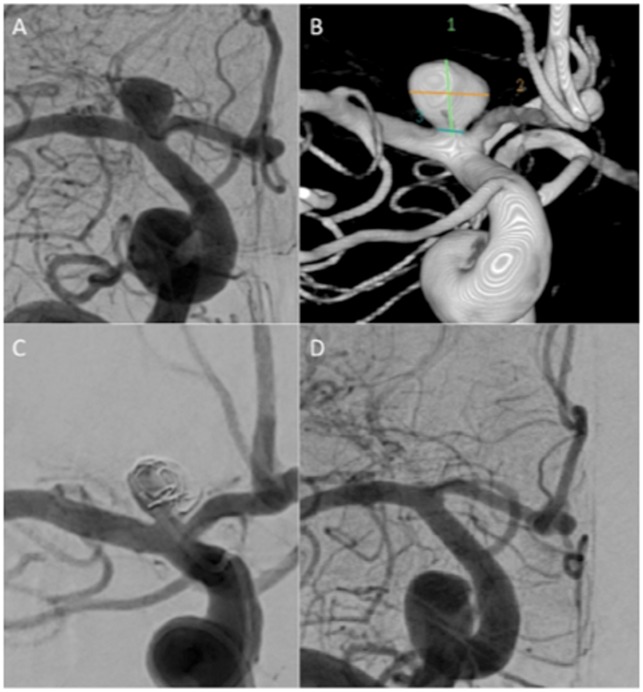
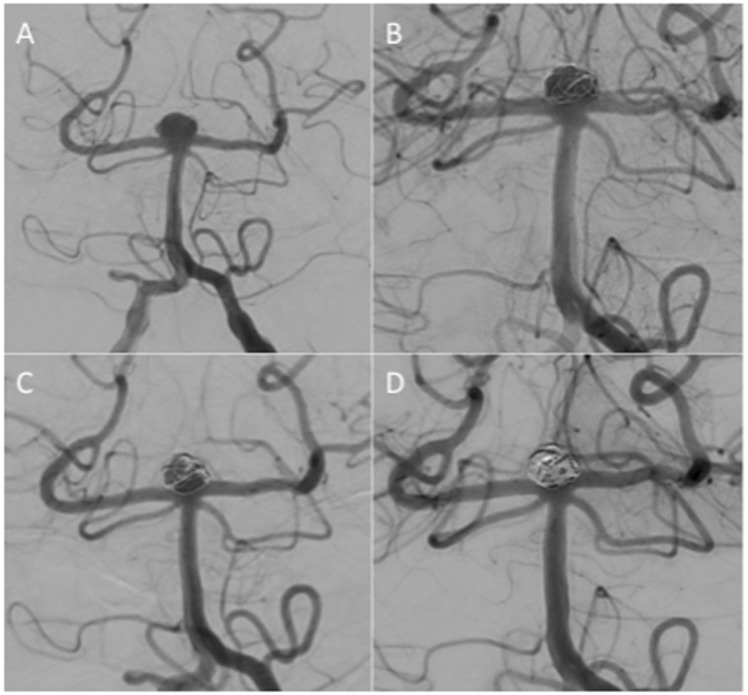
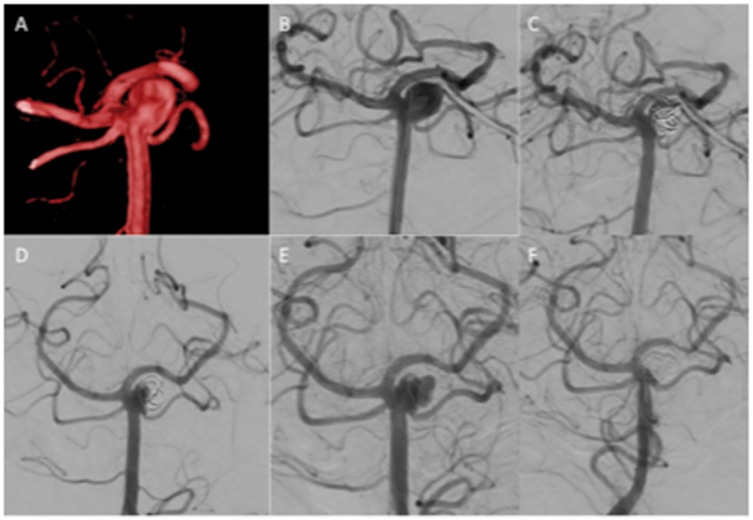
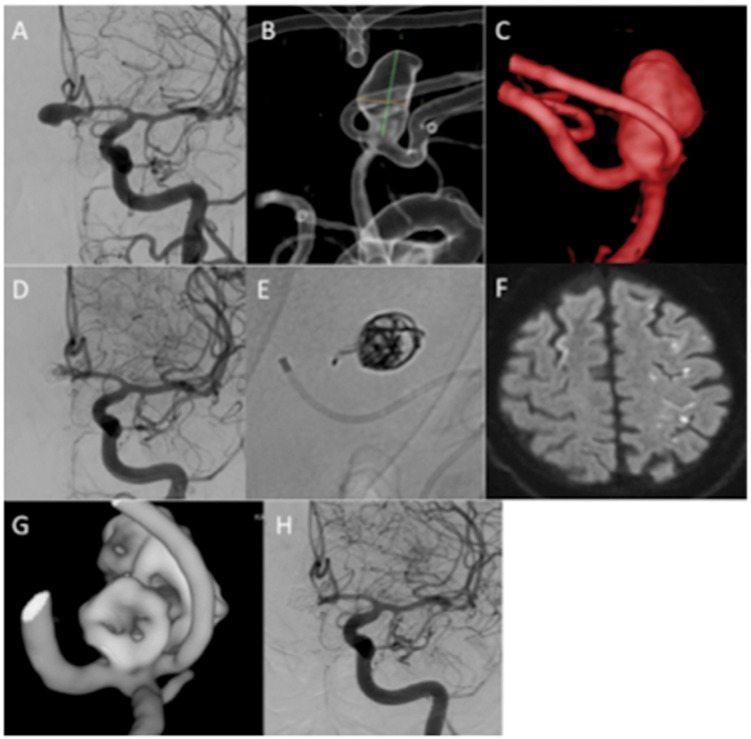
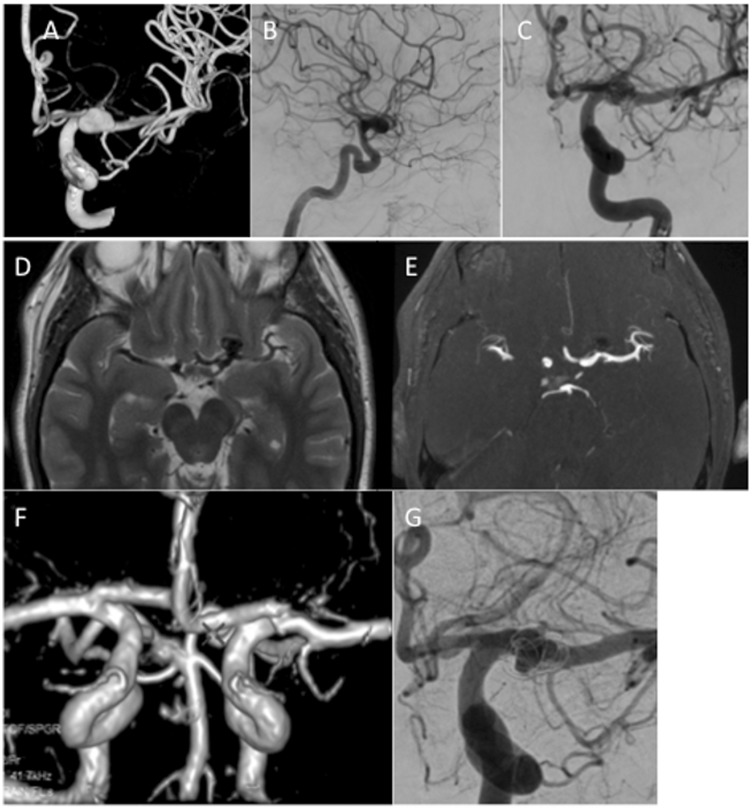
Background The aim of this study was to report our single centre experience with the Medina Embolic Device (MED). Methods We performed a retrospective analysis of prospectively collected data to identify all patients treated with the MED. A total of 14 aneurysms (non-consecutive), in 13 patients, were treated including one ruptured and one partially thrombosed aneurysm. Fundus diameter was ≥5 mm in all cases. We evaluated the angiographic appearances, the clinical status, complications, and the need for adjunctive devices or repeat treatments. Results Aneurysm location was cavernous internal carotid artery (ICA; n = 1), supraclinoid ICA ( n = 1), terminal ICA ( n = 2), anterior communicating artery (AComA; n = 4), A2-3 ( n = 1), M1-2 junction ( n = 1), posterior communicating artery (PComA; n = 1), superior cerebellar artery (SCA; n = 1), and basilar tip ( n = 2). The average aneurysm fundus size was 8.6 mm (range 7-10 mm) and average neck size 3.75 mm (range 1.9-6.9 mm). Immediate angiographic results were modified Raymond-Roy occlusion classification (mRRC) I n = 2, mRRC II n = 1, mRRC IIIa n = 2, mRRC IIIb n = 2, the remaining 7 aneurysms showed complete opacification. At follow-up angiography (mean 5 months) mRRC I n = 5, mRRC II n = 5, mRRC IIIa n = 3, and persistent filling was seen in 1 aneurysm. Overall, four patients had repeat treatment and one is pending further treatment. Of the aneurysms treated with more than one MED, 75% showed complete occlusion at 6-month follow up whereas only one aneurysm treated with a single device showed complete occlusion. Overall, three patients had temporary complications and there were no deaths. Conclusions The MED is an intra-saccular flow-diverting device with satisfactory angiographic results and an acceptable safety profile. Use of a single MED cannot be recommended and further longer term studies are needed prior to widespread clinical use.
Keywords: Aneurysm; Medina Embolic Device; flow diverter; intra-saccular.
Figures

References
-
- Henkes H, Weber W. The past, present and future of endovascular aneurysm treatment. Clin Neuroradiol 2015; 25(Suppl. 2): 317–324. - PubMed
-
- Mascitelli JR, Moyle H, Oermann EK, et al. An update to the Raymond–Roy Occlusion Classification of intracranial aneurysms treated with coil embolization. J Neurointerventional Surg 2015; 7: 496–502. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
