

Appropriate management of asymptomatic carotid stenosis
- PMID: 28959466
- PMCID: PMC5435189
- DOI: 10.1136/svn-2016-000016
Appropriate management of asymptomatic carotid stenosis
Abstract
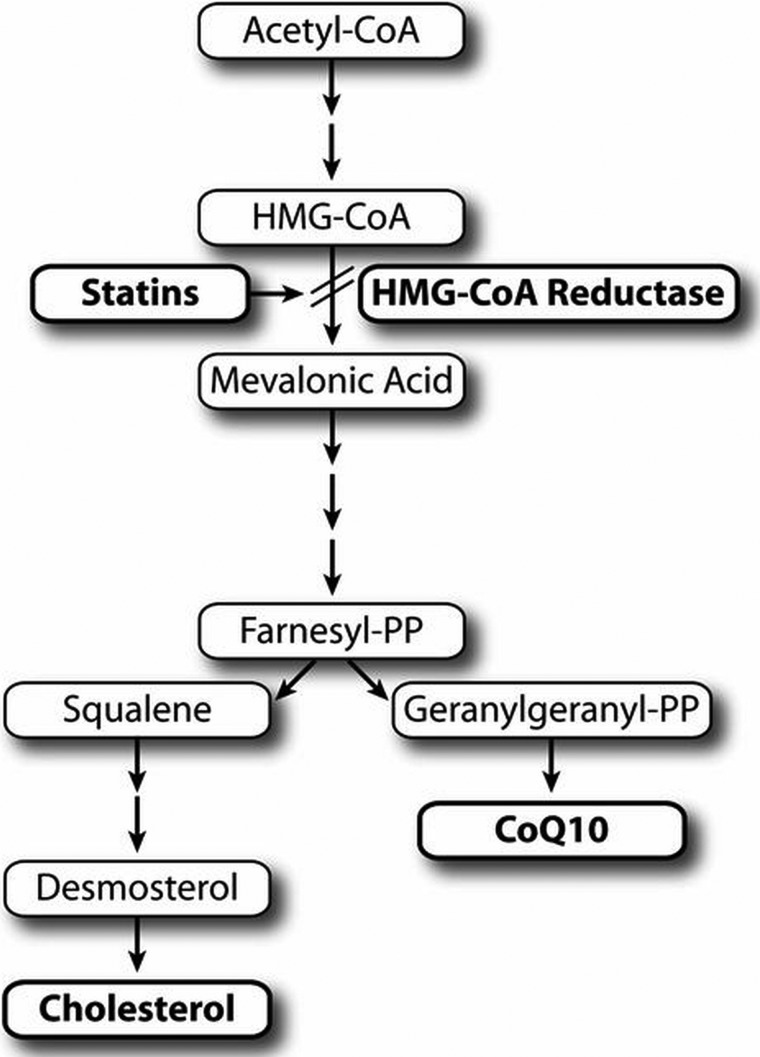
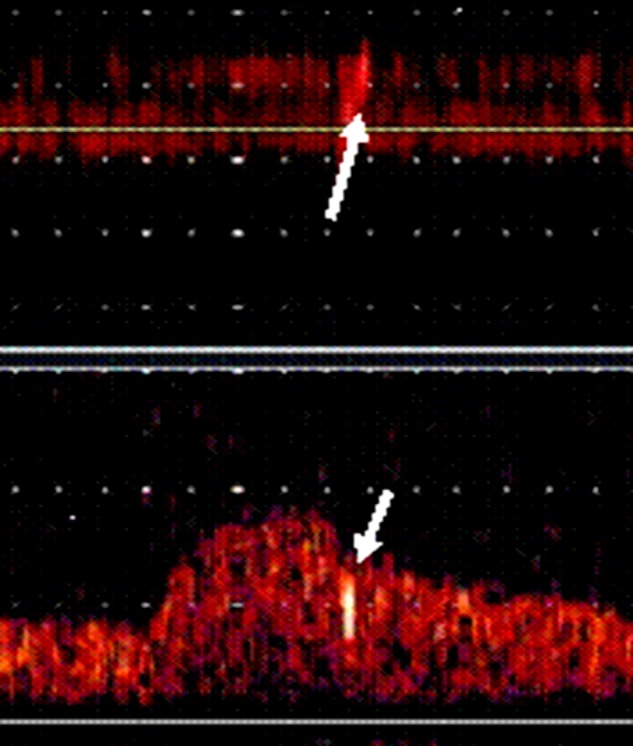
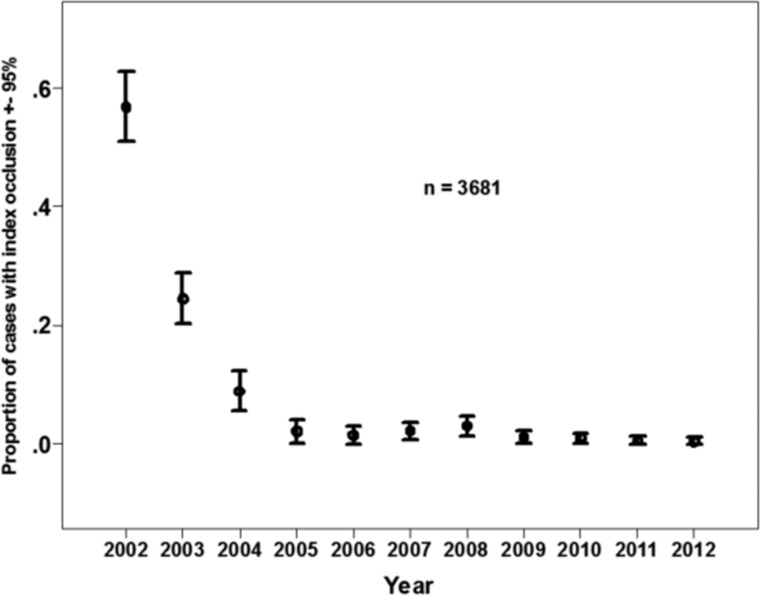
With modern intensive medical therapy, the annual risk of ipsilateral stroke in patients with asymptomatic carotid stenosis (ACS) is now down to ∼0.5%. Despite this, there is a widespread practice of routine intervention in ACS with carotid endarterectomy (CEA) and stenting (CAS). This is being justified on the basis of much higher risks with medical therapy in trials conducted decades ago, compared with lower risks of intervention in recent trials with no medical arm. Such extrapolations are invalid. Although recent trials have shown that after subtracting periprocedural risks the outcomes with CEA and CAS are now comparable to medical therapy, the periprocedural risks still far outweigh the risks with medical therapy. In the asymptomatic carotid trial (ACT) 1 trial, the 30-day risk of stroke or death was 2.9% with CAS and 1.7% with CEA. In the CREST trial, the 30-day risk of stroke or death among asymptomatic patients was 2.5% for stenting and 1.4% for endarterectomy. Thus, intensive medical therapy is much safer than either CAS or CEA. The only patients with ACS who should receive intervention are those who can be identified as being at high risk. The best validated method is transcranial Doppler embolus detection. Other approaches in development for identifying vulnerable plaques include intraplaque haemorrhage on MRI, ulceration and plaque lucency on ultrasound, and plaque inflammation on positron emission tomography/CT. Intensive medical therapy for ACS includes smoking cessation, a Mediterranean diet, effective blood pressure control, antiplatelet therapy, intensive lipid-lowering therapy and treatment with B vitamins (with methylcobalamin instead of cyanocobalamin), particularly in patients with metabolic B12 deficiency. A new strategy called 'treating arteries instead of risk factors', based on measurement of carotid plaque volume, is promising but requires validation in randomised trials.
Keywords: Endarterectomy; Medical therapy; Stenting; Transcranial Doppler; carotid stenosis.
Conflict of interest statement
Competing interests: None declared.
Figures

Similar articles
-
Endarterectomy vs. stenting vs. medical therapy.Int J Stroke. 2016 Jul;11(5):500-1. doi: 10.1177/1747493016643552. Epub 2016 Apr 11. Int J Stroke. 2016. PMID: 27256474
-
Carotid Endarterectomy versus Carotid Stenting or Best Medical Treatment in Asymptomatic Patients with Significant Carotid Stenosis: A meta-analysis.Cardiovasc Revasc Med. 2019 May;20(5):413-423. doi: 10.1016/j.carrev.2018.07.003. Epub 2018 Jul 6. Cardiovasc Revasc Med. 2019. PMID: 30057288
-
Misconceptions regarding the adequacy of best medical intervention alone for asymptomatic carotid stenosis.J Vasc Surg. 2020 Jan;71(1):257-269. doi: 10.1016/j.jvs.2019.04.490. Epub 2019 Sep 26. J Vasc Surg. 2020. PMID: 31564585
-
Transcranial Doppler monitoring for microemboli: a marker of a high-risk carotid plaque.Semin Vasc Surg. 2017 Mar;30(1):62-66. doi: 10.1053/j.semvascsurg.2017.04.011. Epub 2017 Apr 27. Semin Vasc Surg. 2017. PMID: 28818260 Review.
-
Best Medical Therapy for Asymptomatic Carotid Stenosis: Imminent or Ineffective?Ann Vasc Surg. 2025 Apr;113:294-297. doi: 10.1016/j.avsg.2024.09.040. Epub 2024 Sep 29. Ann Vasc Surg. 2025. PMID: 39353486 Review.
Cited by
-
Gray-Scale Median in Patients with Symptomatic and Asymptomatic Carotid Atherosclerosis-Risk Factors and Diagnostic Potential.Biomedicines. 2024 Jul 17;12(7):1594. doi: 10.3390/biomedicines12071594. Biomedicines. 2024. PMID: 39062167 Free PMC article.
-
Poster Viewing Sessions PA00-A01 to PA00-A49.J Cereb Blood Flow Metab. 2019 Jul;39(1_suppl):124-166. doi: 10.1177/0271678X19851017. J Cereb Blood Flow Metab. 2019. PMID: 31265792 Free PMC article. No abstract available.
-
Adaptive Wall Shear Stress Imaging in Phantoms, Simulations and In Vivo.IEEE Trans Biomed Eng. 2023 Jan;70(1):154-165. doi: 10.1109/TBME.2022.3186854. Epub 2022 Dec 26. IEEE Trans Biomed Eng. 2023. PMID: 35776824 Free PMC article.
-
Diagnosis of extracranial carotid stenosis by MRA of the brain.Sci Rep. 2021 Jun 8;11(1):12010. doi: 10.1038/s41598-021-91511-w. Sci Rep. 2021. PMID: 34103593 Free PMC article. Clinical Trial.
-
Carotid artery stenosis and inflammatory biomarkers: the role of inflammation-induced immunological responses affecting the vascular systems.Ann Transl Med. 2020 Oct;8(19):1276. doi: 10.21037/atm-20-4388. Ann Transl Med. 2020. PMID: 33178808 Free PMC article. Review.
References
-
- Spence JD. Measurement of carotid plaque burden. JAMA Neurol 2015;72:383–4. doi:10.1001/jamaneurol.2014.3002 - DOI - PubMed
-
- Chimowitz MI, Weiss DG, Cohen SL, et al. . Cardiac prognosis of patients with carotid stenosis and no history of coronary artery disease. Veterans Affairs Cooperative Study Group 167. Stroke 1994;25:759–65. doi:10.1161/01.STR.25.4.759 - DOI - PubMed
-
- Chiuve SE, Rexrode KM, Spiegelman D, et al. . Primary prevention of stroke by healthy lifestyle. Circulation 2008;118:947–54. doi:10.1161/CIRCULATIONAHA.108.781062 - DOI - PMC - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. . Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation 2015;131:e29–322. doi:10.1161/CIR.0000000000000152 - DOI - PubMed
-
- Larsson SC, Akesson A, Wolk A. Healthy diet and lifestyle and risk of stroke in a prospective cohort of women. Neurology 2014;83:1699–704. doi:10.1212/WNL.0000000000000954 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources