

Update on cerebral small vessel disease: a dynamic whole-brain disease
- PMID: 28959468
- PMCID: PMC5435198
- DOI: 10.1136/svn-2016-000035
Update on cerebral small vessel disease: a dynamic whole-brain disease
Abstract
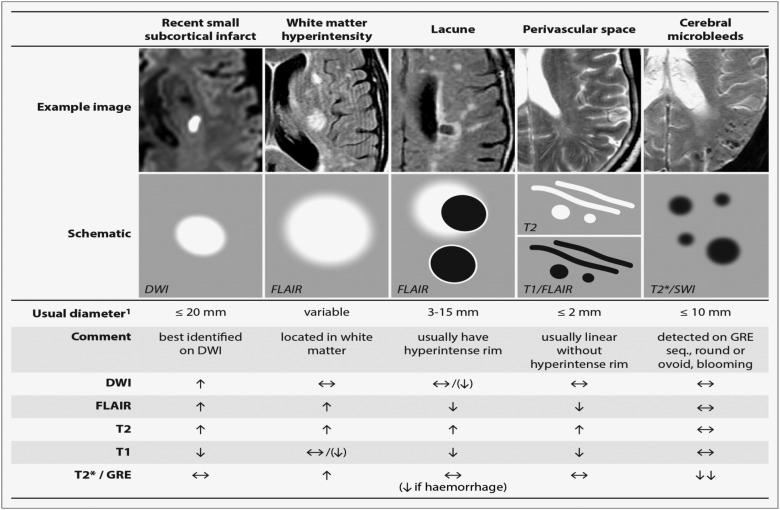
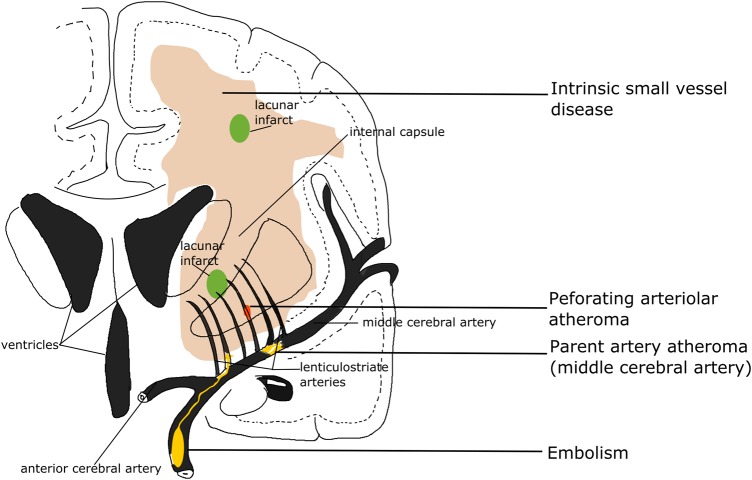
Cerebral small vessel disease (CSVD) is a very common neurological disease in older people. It causes stroke and dementia, mood disturbance and gait problems. Since it is difficult to visualise CSVD pathologies in vivo, the diagnosis of CSVD has relied on imaging findings including white matter hyperintensities, lacunar ischaemic stroke, lacunes, microbleeds, visible perivascular spaces and many haemorrhagic strokes. However, variations in the use of definition and terms of these features have probably caused confusion and difficulties in interpreting results of previous studies. A standardised use of terms should be encouraged in CSVD research. These CSVD features have long been regarded as different lesions, but emerging evidence has indicated that they might share some common intrinsic microvascular pathologies and therefore, owing to its diffuse nature, CSVD should be regarded as a 'whole-brain disease'. Single antiplatelet (for acute lacunar ischaemic stroke) and management of traditional risk factors still remain the most important therapeutic and preventive approach, due to limited understanding of pathophysiology in CSVD. Increasing evidence suggests that new studies should consider drugs that target endothelium and blood-brain barrier to prevent and treat CSVD. Epidemiology of CSVD might differ in Asian compared with Western populations (where most results and guidelines about CSVD and stroke originate), but more community-based data and clear stratification of stroke types are required to address this.
Keywords: Blood Brain Barrier; Cerebral Small Vessel Disease; Lacunar Infarct; Microvascular dysfunction; White Matter Hyperintensities.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol 2010;9:689–701. doi:10.1016/S1474-4422(10)70104-6 - DOI - PubMed
-
- Tsai CF, Thomas B, Sudlow CL. Epidemiology of stroke and its subtypes in Chinese vs white populations: a systematic review. Neurology 2013;81:264–72. doi:10.1212/WNL.0b013e31829bfde3 - DOI - PMC - PubMed
-
- Fang XH, Wang WH, Zhang XQ, et al. Incidence and survival of symptomatic lacunar infarction in a Beijing population: a 6-year prospective study. Eur J Neurol 2012;19:1114–20. doi:10.1111/j.1468-1331.2012.03709.x - DOI - PubMed
-
- Wardlaw JM, Smith EE, Biessels GJ, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol 2013;12:822–38. doi:10.1016/S1474-4422(13)70124-8 - DOI - PMC - PubMed
-
- Vermeer SE, Longstreth WT Jr, Koudstaal PJ. Silent brain infarcts: a systematic review. Lancet Neurol 2007;6:611–19. doi:10.1016/S1474-4422(07)70170-9 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources