

Prevalence and Clinical Characteristics of Metabolically Healthy Obesity in Korean Children and Adolescents: Data from the Korea National Health and Nutrition Examination Survey
- PMID: 28960038
- PMCID: PMC5639066
- DOI: 10.3346/jkms.2017.32.11.1840
Prevalence and Clinical Characteristics of Metabolically Healthy Obesity in Korean Children and Adolescents: Data from the Korea National Health and Nutrition Examination Survey
Abstract
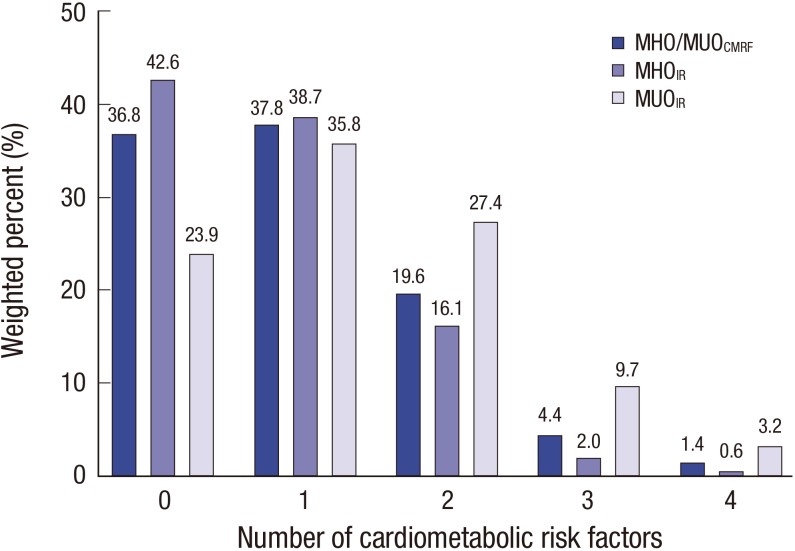
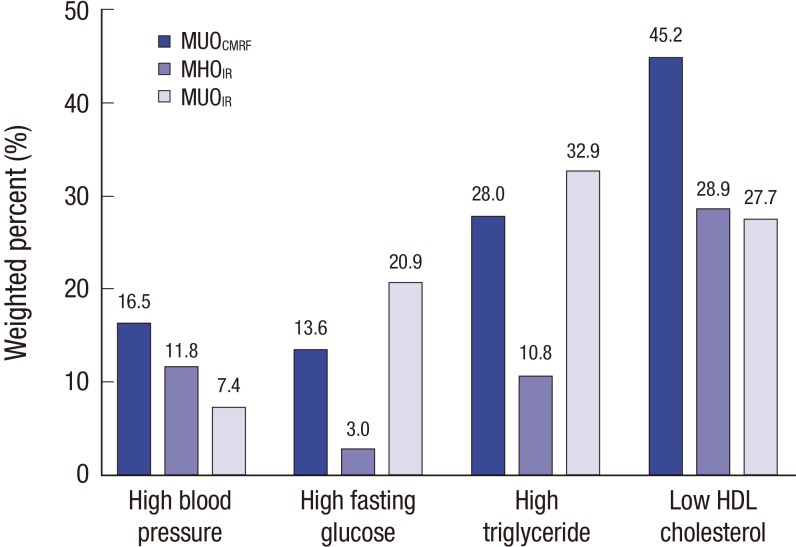
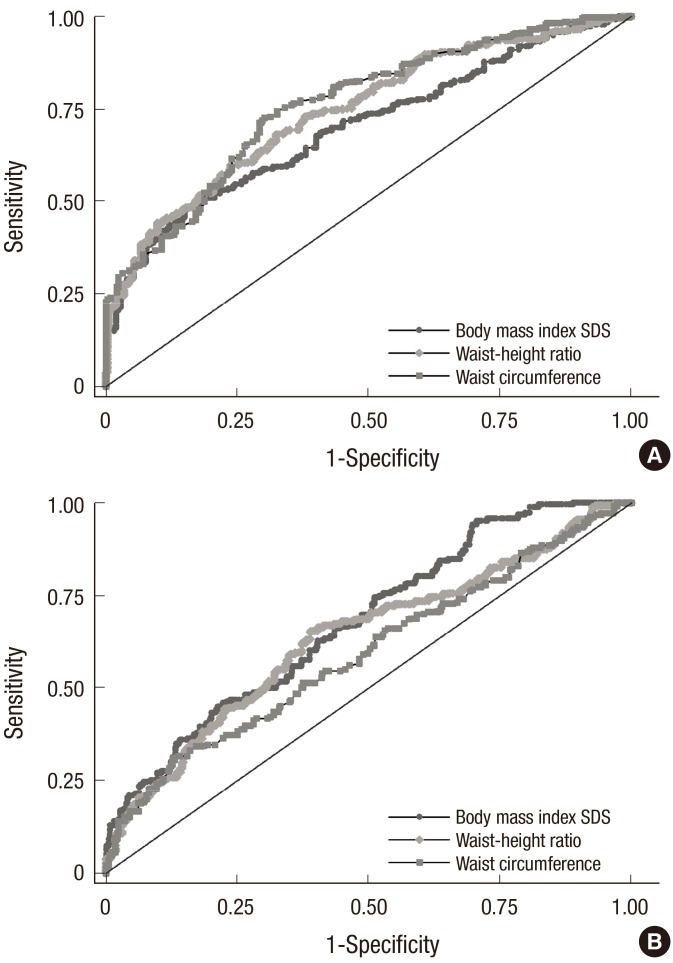
Metabolically healthy obesity (MHO) and metabolically unhealthy obesity (MUO) are differentiated by the presence of cardiometabolic risk factors (CMRFs) and insulin resistance (IR). This study aimed to evaluate the prevalence and clinical characteristics of MHO in Korean children and adolescents and to investigate the anthropometric, laboratory, and lifestyle predictors of MHO. This study included data from 530 obese subjects, aged 10-19 years, obtained from the Fourth Korea National Health and Nutrition Examination Survey. Subjects were classified into MHO and MUO groups according to the presence of CMRF (MHO(CMRF)/MUO(CMRF)) and degree of IR (MHO(IR)/MUO(IR)). Demographic, anthropometric, cardiometabolic, and lifestyle factors were compared between the groups. Logistic regression analysis and receiver operating characteristic curve analysis were performed to identify factors that predicted MHO. The prevalence of MHO(CMRF) and MHO(IR) in obese Korean youth was 36.8% (n = 197) and 68.8% (n = 356), respectively. CMRF profiles were significantly less favorable in MUO children. Longer and more vigorous physical activity and less protein intake were associated with MHO(CMRF) phenotype. The best predictors of MHO(CMRF) and MHO(IR) were waist circumference (odds ratio [OR], 0.82; 95% confidence interval [CI], 0.77-0.88; P < 0.001) and body mass index (BMI) standard deviation score (OR, 0.24; 95% CI, 0.15-0.39; P < 0.001), respectively. The prevalence of MHO differed depending on how it was defined. To adequately manage obesity in youth, the approach to individuals with MHO and MUO should be personalized due to variation in clinical characteristics. Longitudinal studies are needed to evaluate long-term consequences of MHO.
Keywords: Children; Korea; Metabolically Healthy Obesity; Prevalence.
© 2017 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Comparison between metabolically healthy obesity and metabolically unhealthy obesity by different definitions among Mexican children.J Pediatr Endocrinol Metab. 2020 Feb 25;33(2):215-222. doi: 10.1515/jpem-2019-0077. J Pediatr Endocrinol Metab. 2020. PMID: 31834862
-
Utility of obesity indicators for metabolically healthy obesity: an observational study using the Korean National Health and Nutrition Examination Survey (2009-2010).BMC Public Health. 2014 Nov 14;14:1166. doi: 10.1186/1471-2458-14-1166. BMC Public Health. 2014. PMID: 25394775 Free PMC article.
-
Cardiovascular Risk Factors Associated With the Metabolically Healthy Obese (MHO) Phenotype Compared to the Metabolically Unhealthy Obese (MUO) Phenotype in Children.Front Endocrinol (Lausanne). 2020 Feb 7;11:27. doi: 10.3389/fendo.2020.00027. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32117055 Free PMC article.
-
Epidemiology and pathophysiology of the association between NAFLD and metabolically healthy or metabolically unhealthy obesity.Ann Hepatol. 2020 Jul-Aug;19(4):359-366. doi: 10.1016/j.aohep.2020.03.001. Epub 2020 Mar 21. Ann Hepatol. 2020. PMID: 32349939 Review.
-
The Definition and Prevalence of Obesity and Metabolic Syndrome: Correlative Clinical Evaluation Based on Phenotypes.Adv Exp Med Biol. 2024;1460:1-25. doi: 10.1007/978-3-031-63657-8_1. Adv Exp Med Biol. 2024. PMID: 39287847 Review.
Cited by
-
Children with metabolically healthy obesity have a worse metabolic profile compared to normal-weight peers: a cross-sectional study.Endocrine. 2021 Sep;73(3):580-587. doi: 10.1007/s12020-021-02762-6. Epub 2021 May 22. Endocrine. 2021. PMID: 34023981
-
Dietary intake and nutritional status of Korean children and adolescents: a review of national survey data.Clin Exp Pediatr. 2021 Sep;64(9):443-458. doi: 10.3345/cep.2020.01655. Epub 2020 Dec 28. Clin Exp Pediatr. 2021. PMID: 33445834 Free PMC article.
-
Prevalence and associated factors of metabolic body size phenotype in children and adolescents: A national cross-sectional analysis in China.Front Endocrinol (Lausanne). 2022 Aug 25;13:952825. doi: 10.3389/fendo.2022.952825. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36093090 Free PMC article.
-
Metabolically Healthy Obesity.Endocr Rev. 2020 May 1;41(3):bnaa004. doi: 10.1210/endrev/bnaa004. Endocr Rev. 2020. PMID: 32128581 Free PMC article. Review.
-
Prevalence and predictors of metabolically healthy obesity in severely obese Asian children.Pediatr Res. 2022 Nov;92(5):1374-1380. doi: 10.1038/s41390-022-01941-z. Epub 2022 Feb 7. Pediatr Res. 2022. PMID: 35132129
References
-
- Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, Biryukov S, Abbafati C, Abera SF, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. - PMC - PubMed
-
- Oh K, Jang MJ, Lee NY, Moon JS, Lee CG, Yoo MH, Kim YT. Prevalence and trends in obesity among Korean children and adolescents in 1997 and 2005. Korean J Pediatr. 2008;51:950–955.
-
- Reilly JJ. Descriptive epidemiology and health consequences of childhood obesity. Best Pract Res Clin Endocrinol Metab. 2005;19:327–341. - PubMed
-
- Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity: public-health crisis, common sense cure. Lancet. 2002;360:473–482. - PubMed
-
- Sims EA. Are there persons who are obese, but metabolically healthy? Metabolism. 2001;50:1499–1504. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
