

Multiple switches between GP2015, an etanercept biosimilar, with originator product do not impact efficacy, safety and immunogenicity in patients with chronic plaque-type psoriasis: 30-week results from the phase 3, confirmatory EGALITY study
- PMID: 28960486
- PMCID: PMC5887937
- DOI: 10.1111/jdv.14605
Multiple switches between GP2015, an etanercept biosimilar, with originator product do not impact efficacy, safety and immunogenicity in patients with chronic plaque-type psoriasis: 30-week results from the phase 3, confirmatory EGALITY study
Abstract
Background: EGALITY was a phase III confirmatory efficacy and safety study conducted in patients with plaque-type psoriasis as a part of totality of evidence gathered during the development of GP2015, an etanercept biosimilar.
Objective: To demonstrate equivalent efficacy and comparable safety and immunogenicity of GP2015 and the etanercept originator product (ETN, Enbrel® ) and evaluate effects of repeated switching between GP2015 and ETN. Results for efficacy, safety and immunogenicity during treatment period (TP) 2 (TP2) are presented pooling the two continued treatment arms (pooled continued) versus the two treatment arms with repeated switches (pooled switched).
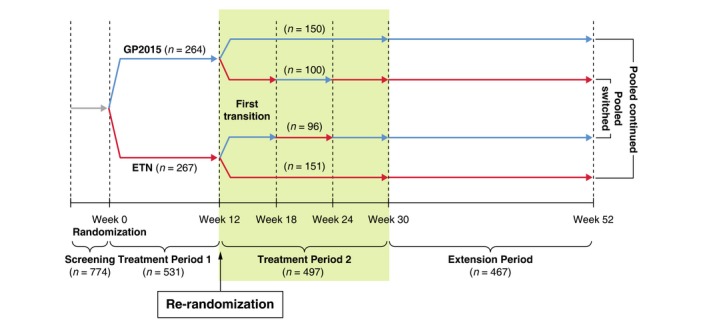
Methods: Patients (n = 531) were randomized 1:1 to self-administer GP2015 or ETN twice-weekly subcutaneously during TP1. Patients with a ≥50% improvement in Psoriasis Area and Severity Index (PASI 50) at week 12 were re-randomized for TP2 to continue the same treatment at once-weekly dosing or to undergo three consecutive treatment switches between GP2015 and ETN until week 30. Patients continued the last-assigned treatment during TP2, until week 52.
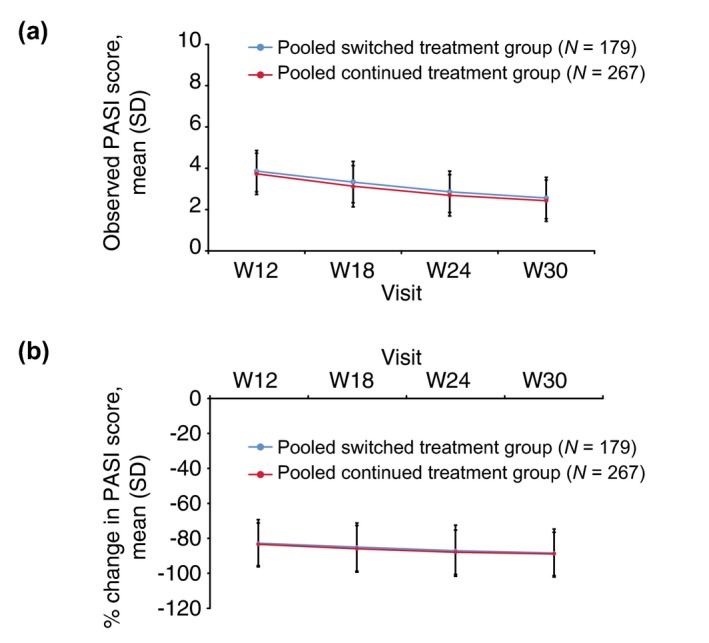
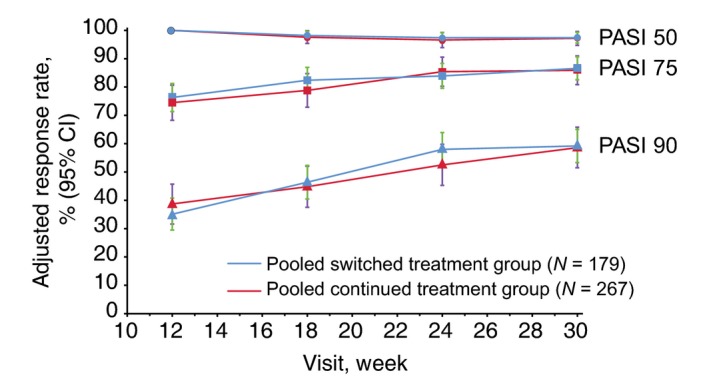
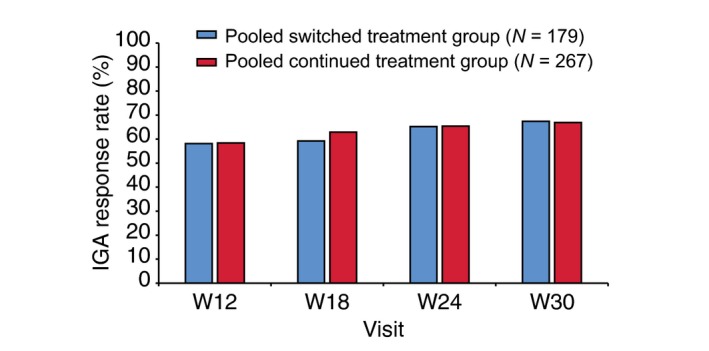
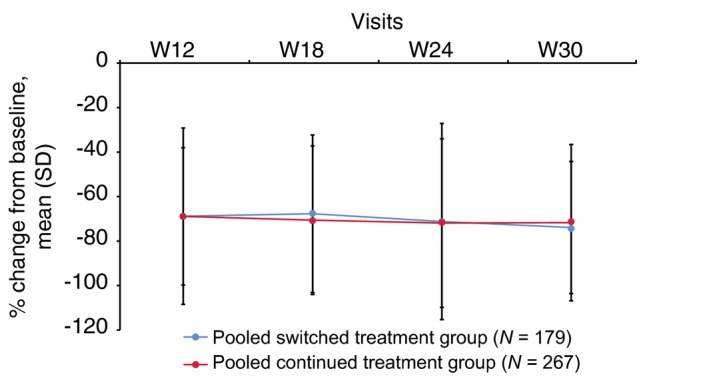
Results: Mean (standard deviation [SD]) PASI scores at baseline were similar in patients who underwent multiple switches compared to those with continued treatments during TP2. During TP2, PASI 50, PASI 75 and PASI 90 response rates, percent change from baseline in PASI scores and all other efficacy parameters were similar between the pooled switched and pooled continued treatment groups at all time points. The incidence of treatment-emergent adverse events including injection site reactions was comparable between the pooled switched (36.7%) and pooled continued (34.9%) groups. None of the patients in either treatment group were positive for binding anti-drug antibodies in TP2.
Conclusion: Treatment efficacy, safety and immunogenicity were similar between the pooled continued and pooled switched treatments during TP2, indicating that there are no effects in the short term on clinical data of multiple switches between GP2015 and ETN.
© 2017 The Authors. Journal of the European Academy of Dermatology and Venereology published by John Wiley & Sons Ltd on behalf of European Academy of Dermatology and Venereology.
Figures
References
-
- Daller J. Biosimilars: a consideration of the regulations in the United States and European union. Regul Toxicol Pharmacol 2016; 76: 199–208. - PubMed
-
- USFDA . Scientific considerations in demonstrating biosimilarity to a reference product ‐ Guidance for industry. Last updated on 2015. http://www.fda.gov/ucm/groups/fdagov-public/@fdagov-drugs-gen/documents/... (last accessed on Feb 06, 2017).
-
- European Medicines Agency . Guideline on similar biological medicinal products containing biotechnology‐derived proteins as active substance: non‐clinical and clinical issues. 2014. Last updated on December 18, 2014. URL: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2015/01/WC500180219.pdf (last accessed: Feb 06, 2017).
-
- Kay J. Editorial: biosimilars: new or Deja Vu? Arthritis Rheumatol 2016; 68: 1049–1052. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
