

Biomechanical Stability Analysis of a Stand-alone Cage, Static and Rotational-dynamic Plate in a Two-level Cervical Fusion Construct
- PMID: 28960818
- PMCID: PMC6584158
- DOI: 10.1111/os.12339
Biomechanical Stability Analysis of a Stand-alone Cage, Static and Rotational-dynamic Plate in a Two-level Cervical Fusion Construct
Abstract
Objective: To test the following hypotheses: (i) anterior cervical discetomy and fusion (ACDF) using stand-alone interbody spacers will significantly reduce the range of motion from intact spine; and (ii) the use of a static or a rotational-dynamic plate will significantly augment the stability of stand-alone interbody spacers, with similar beneficial effect when compared to each other.
Methods: Eleven human cadaveric subaxial cervical spines (age: 48.2 ± 5.4 years) were tested under the following sequence: (i) intact spine; (ii) ACDF at C4 -C5 using a stand-alone interbody spacer; (iii) ACDF at C5 -C6 and insertion of an interbody spacer (two-level construct); and (iv) randomized placement of either a two-level locking static plate or a rotational-dynamic plate.
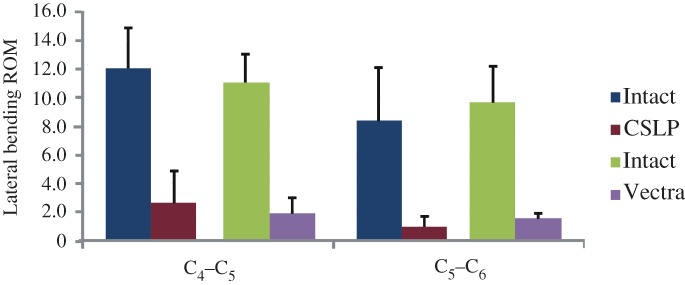
Results: Insertion of stand-alone cage at C4 -C5 and C5 -C6 caused a significant decrease in the range of motion compared to intact spine (P < 0.05). Placement of both the locking and the rotational dynamic plate further reduced the range of motion at C4 -C5 and C5 -C6 compared to stand-alone cage (P < 0.01). No significant differences in range of motion restriction at either C4 -C5 or C5 -C6 were found when the two plating systems were compared (P > 0.05).
Conclusions: Cervical stand-alone interbody spacers caused significant restriction in the range of motion. Both plates significantly augmented the stability of stand-alone interbody spacers, with similar stabilizing effect.
Keywords: Anterior cervical discectomy and fusion; Biomechanics; Plating; Range of motion; Stand-alone cages.
© 2017 Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures







References
-
- Anderson DG, Albert TJ. Bone grafting, implants, and plating options for anterior cervical fusions. Orthop Clin North Am, 2002, 33: 317–328. - PubMed
-
- Mastronardi L, Ducati A, Ferrante L. Anterior cervical fusion with polyetheretherketone (PEEK) cages in the treatment of degenerative disc disease. Preliminary observations in 36 consecutive cases with a minimum 12‐month follow‐up. Acta Neurochir (Wien), 2006, 148: 307–312. - PubMed
-
- Cho DY, Lee WY, Sheu PC. Treatment of multilevel cervical fusion with cages. Surg Neurol, 2004, 62: 378–385. - PubMed
-
- Profeta G, de Falco R, Ianniciello G, Profeta L, Cigliano A, Raja AI. Preliminary experience with anterior cervical microdiscectomy and interbody titanium cage fusion (Novus CT‐Ti) in patients with cervical disc disease. Surg Neurol, 2000, 53: 417–426. - PubMed
-
- Moon HJ, Kim JH, Kwon TH, Chung HS, Park YK. The effects of anterior cervical discectomy and fusion with stand‐alone cages at two contiguous levels on cervical alignment and outcomes. Acta Neurochir (Wien), 2011, 153: 559–565. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
