

Introducing leprosy post-exposure prophylaxis into the health systems of India, Nepal and Indonesia: a case study
- PMID: 28962564
- PMCID: PMC5622547
- DOI: 10.1186/s12913-017-2611-7
Introducing leprosy post-exposure prophylaxis into the health systems of India, Nepal and Indonesia: a case study
Abstract
Background: Leprosy has a wide range of clinical and socio-economic consequences. India, Indonesia and Nepal contribute significantly to the global leprosy burden. After integration, the health systems are pivotal in leprosy service delivery. The Leprosy Post Exposure Prophylaxis (LPEP) program is ongoing to investigate the feasibility of providing single dose rifampicin (SDR) as post-exposure prophylaxis (PEP) to the contacts of leprosy cases in various health systems. We aim to compare national leprosy control programs, and adapted LPEP strategies in India, Nepal and Indonesia. The purpose is to establish a baseline of the health system's situation and document the subsequent adjustment of LPEP, which will provide the context for interpreting the LPEP results in future.
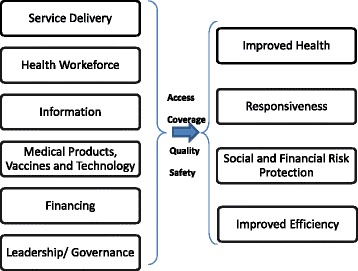
Methods: The study followed the multiple-case study design with single units of analysis. The data collection methods were direct observation, in-depth interviews and desk review. The study was divided into two phases, i.e. review of national leprosy programs and description of the LPEP program. The comparative analysis was performed using the WHO health system frameworks (2007).
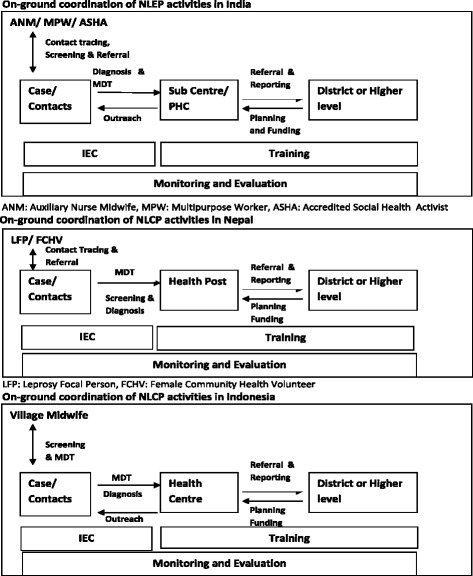
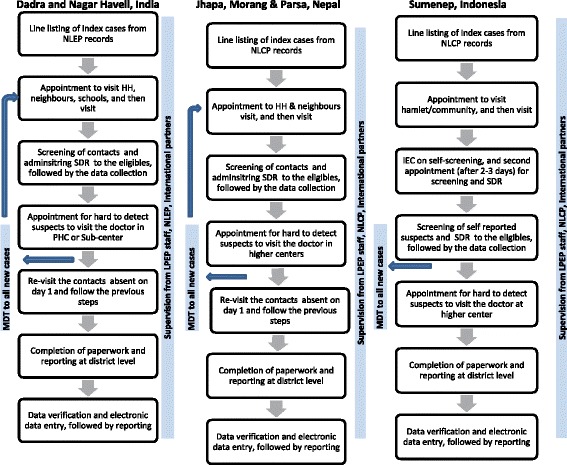
Results: In all countries leprosy services including contact tracing is integrated into the health systems. The LPEP program is fully integrated into the established national leprosy programs, with SDR and increased documentation, which need major additions to standard procedures. PEP administration was widely perceived as well manageable, but the additional LPEP data collection was reported to increase workload in the first year.
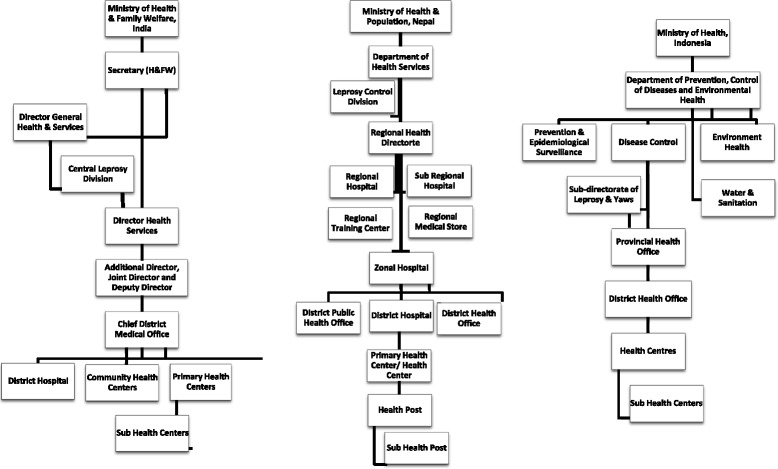
Conclusions: The findings of our study led to the recommendation that field-based leprosy research programs should keep health systems in focus. The national leprosy programs are diverse in terms of organizational hierarchy, human resource quantity and capacity. We conclude that PEP can be integrated into different health systems without major structural and personal changes, but provisions are necessary for the additional monitoring requirements.
Keywords: Chemoprophylaxis; Health systems; Leprosy; National Leprosy Control Programs.
Conflict of interest statement
Ethics approval and consent to participate
This study was conducted under the LPEP program. The ethics approval for LPEP was obtained from the Institutional Human Ethics Committee, National Institute of Epidemiology, Indian Council of Medical Research (NIE/IHEC/201407–01) and Ethical Review Board, Nepal Health Research Council (NHRC 39/2015). There was no need for ethical clearance in Indonesia as post exposure prophylaxis was already a part of national leprosy control strategy. A verbal consent was sought from the respondents. No individual identifiable data were recorded.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Country Leadership and Collaboration on Neglected Tropical Diseases: Third progress report of the London Declaration. http://unitingtocombatntds.org/sites/default/files/resource_file/london_.... Accessed 9 Nov 2016.
-
- Global leprosy update, 2014: need for early case detection. Wkly Epidemiol Rec. 2015;90(36):461–74. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
