

Assessment of intracranial pressure with ultrasonographic retrobulbar optic nerve sheath diameter measurement
- PMID: 28962603
- PMCID: PMC5622417
- DOI: 10.1186/s12883-017-0964-5
Assessment of intracranial pressure with ultrasonographic retrobulbar optic nerve sheath diameter measurement
Abstract
Background: Ultrasonograpic retrobulbar optic nerve sheath diameter (ONSD) measurement is considered to be an alternative noninvasive method to estimate intracranial pressure,but the further validation is urgently needed. The aim of the current study was to investigate the association of the ultrasonographic ONSD and intracranial pressure (ICP) in patients.
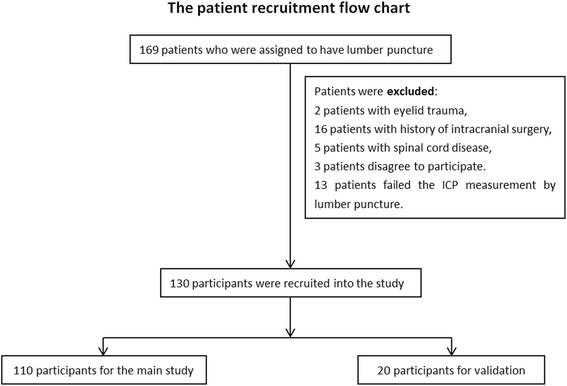
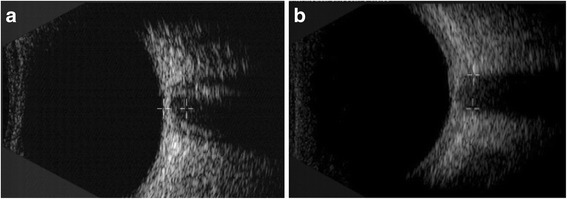
Methods: One hundred and ten patients whose intracranial pressure measured via lumbar puncture were enrolled in the study. Their retrobulbar ONSD with B-scan ultrasound was determined just before lumber puncture. The correlation between the ICP and the body mass index (BMI), ONSD or age was established respectively with the Pearson correlation coefficient analysis. The discriminant analysis was used to obtain a discriminant formula for predicting ICP with the ONSD、BMI、gender and age. Another 20 patients were recruited for further validation the efficiency of this discriminant equation.
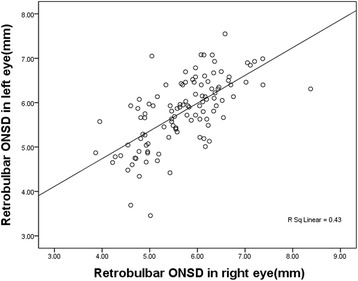
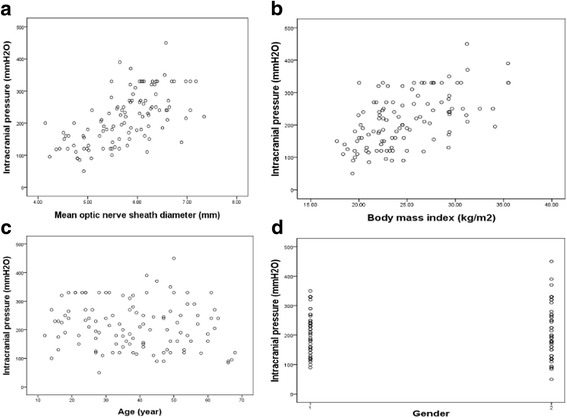
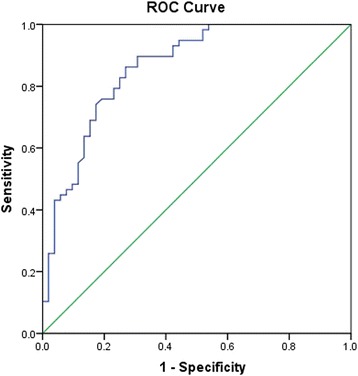
Results: The mean ICP was 215.3 ± 81.2 mmH2O. ONSD was 5.70 ± 0.80 mm in the right eye and 5.80 ± 0.77 mm in the left eye. A significant correlation was found between ICP and BMI (r = 0.554, p < 0.001), the mean ONSD (r = 0.61, P < 0.001), but not with age (r = -0.131, p = 0.174) and gender (r = 0.03, p = 0.753). Using receiver operating characteristic (ROC) curve analysis, the critical value for the risk mean-ONSD was 5.6 mm from the ROC curve, with the sensitivity of 86.2% and specificity of 73.1%. With 200 mmH2O as the cutoff point for a high or low ICP, stepwise discriminant was applied, the sensitivity and specificity of ONSD predicting ICP was 84.5%-85.7% and 86.5%-92.3%.
Conclusions: Ophthalmic ultrasound measurement of ONSD may be a good surrogate of invasive ICP measurement. This non-invasive method may be an alternative approach to predict the ICP value of patients whose ICP measurement via lumbar puncture are in high risk. The discriminant formula, which incorporated the factor of BMI, had similar sensitivity and higher specificity than the ROC curve.
Keywords: B-scan ultrasonography; Intracranial pressure; Optic nerve sheath diameter.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by Ethics Committee of Xuanwu Hospital, Capital Medical University. The number of approval letter was 2,017,003. A written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- F. Gjerris and J. Brennum. The cerebrospinal fluid, intracranial pressure and herniation of the brain. Clinical Neurology and Neurosurgery, O. B. Paulson, F. Gjerris, and P. S. Sørensen, Eds., pp. 179–196, FADL’s ForlagAktieselskab, Copenhagen, Denmark, 2004.
-
- Zeng T, Gao L. Management of patients with severe traumatic brain injury guided by intraventricular intracranial pressure monitoring: a report of 136 cases. Chin J Traumatol. 2010;13(3):146–151. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
