

A population-based incidence of M2 strokes indicates potential expansion of large vessel occlusions amenable to endovascular therapy
- PMID: 28963363
- PMCID: PMC5969390
- DOI: 10.1136/neurintsurg-2017-013371
A population-based incidence of M2 strokes indicates potential expansion of large vessel occlusions amenable to endovascular therapy
Abstract
Background: M2 occlusions may result in poor outcomes and potentially benefit from endovascular therapy. Data on the rate of M2 strokes is lacking.
Methodology: Patients with acute ischemic stroke discharged over a period of 3 years from a tertiary level hospital in the 'stroke belt' were evaluated for M2 occlusions on baseline vascular imaging. Regional and national incidence was calculated from discharge and multicounty data.
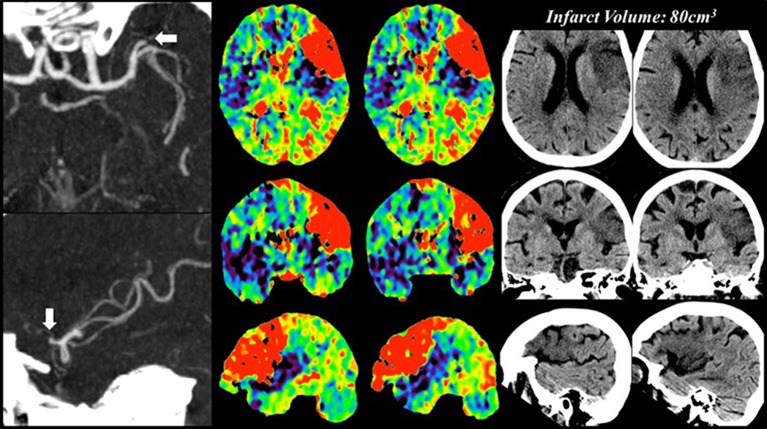
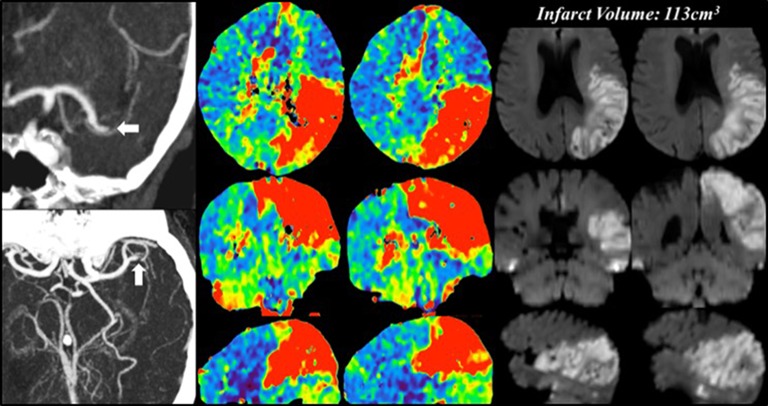
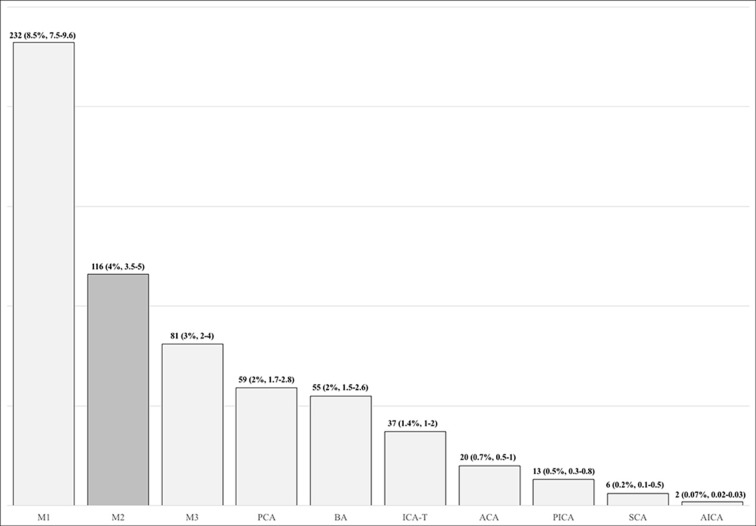
Results: There were 2739 ICD-9 based AIS discharges. M2 occlusions in 116 (4%, 95% CI 3.5% to 5%) patients constituted the second most common occlusion site. The median National Institute of Health Stroke Scale (NIHSS) score was 12 (IQR 5-18). Good outcomes were observed in 43% (95% CI 34% to 53%), poor outcomes in 57% (95% CI 47% to 66%), and death occurred in 27% (95% CI 19% to 37%) of patients. Receiver operating characteristics curves showed the NIHSS to be predictive of outcomes (area under the curve 0.829, 95% CI 0.745 to 0.913, p<0.0001). An NIHSS score ≥9 was the optimal cut-off point for predicting poor outcomes (sensitivity 85.7%, specificity 67.4%). 71 (61%) patients had an NIHSS score ≥9 and 45 (39%) an NIHSS score <9. The rate of good-outcome was 22.6% for NIHSS score ≥9 versus 78.4% for NIHSSscore <9 (OR=0.08, 95% CI 0.03 to 0.21, p<0.0001). Mortality was 42% for NIHSS score ≥9 versus 2.7% for NIHSS score <9 (OR=26, 95% CI 3.3 to 202, p<0.0001). Infarct volume was 57 (±55.7) cm3 for NIHSS score ≥9 versus 30 (±34)cm3 for NIHSS score <9 (p=0.003). IV recombinant tissue plasminogen activator (rtPA) administered in 28 (24%) patients did not affect outcomes. The rate of M2 occlusions was 7 (95% CI 5 to 9)/100 000 people/year (3%, 95% CI 2% to 4%), giving an incidence of 21 176 (95% CI 15 282 to 29 247)/year. Combined with M1, internal carotid artery terminus and basilar artery, this yields a 'large vessel occlusion (LVO)+M2' rate of 31 (95% CI 26 to 35)/100 000 people/year and a national incidence of 99 227 (95% CI 84 004 to 112 005) LVO+M2 strokes/year.
Conclusion: M2 occlusions can present with serious neurological deficits and cause significant morbidity and mortality. Patients with M2 occlusions and higher baseline deficits (NIHSS score ≥9) may benefit from endovascular therapy, thus potentially expanding the category of acute ischemic strokes amenable to intervention.
Keywords: M2; incidence; stroke; thrombectomy.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Rai AT, Seldon AE, Boo S, et al. A population-based incidence of acute large vessel occlusions and thrombectomy eligible patients indicates significant potential for growth of endovascular stroke therapy in the USA. J Neurointerv Surg 2017;9:722–6. 10.1136/neurintsurg-2016-012515 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical