

TREVO stent-retriever mechanical thrombectomy for acute ischemic stroke secondary to large vessel occlusion registry
- PMID: 28963367
- PMCID: PMC5969387
- DOI: 10.1136/neurintsurg-2017-013328
TREVO stent-retriever mechanical thrombectomy for acute ischemic stroke secondary to large vessel occlusion registry
Abstract
Background: Recent randomized clinical trials (RCTs) demonstrated the efficacy of mechanical thrombectomy using stent-retrievers in patients with acute ischemic stroke (AIS) with large vessel occlusions; however, it remains unclear if these results translate to a real-world setting. The TREVO Stent-Retriever Acute Stroke (TRACK) multicenter Registry aimed to evaluate the use of the Trevo device in everyday clinical practice.
Methods: Twenty-three centers enrolled consecutive AIS patients treated from March 2013 through August 2015 with the Trevo device. The primary outcome was defined as achieving a Thrombolysis in Cerebral Infarction (TICI) score of ≥2b. Secondary outcomes included 90-day modified Rankin Scale (mRS), mortality, and symptomatic intracranial hemorrhage (sICH).
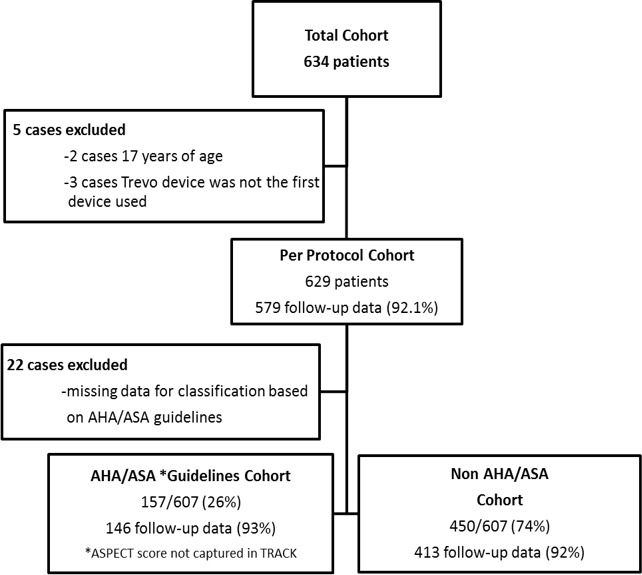
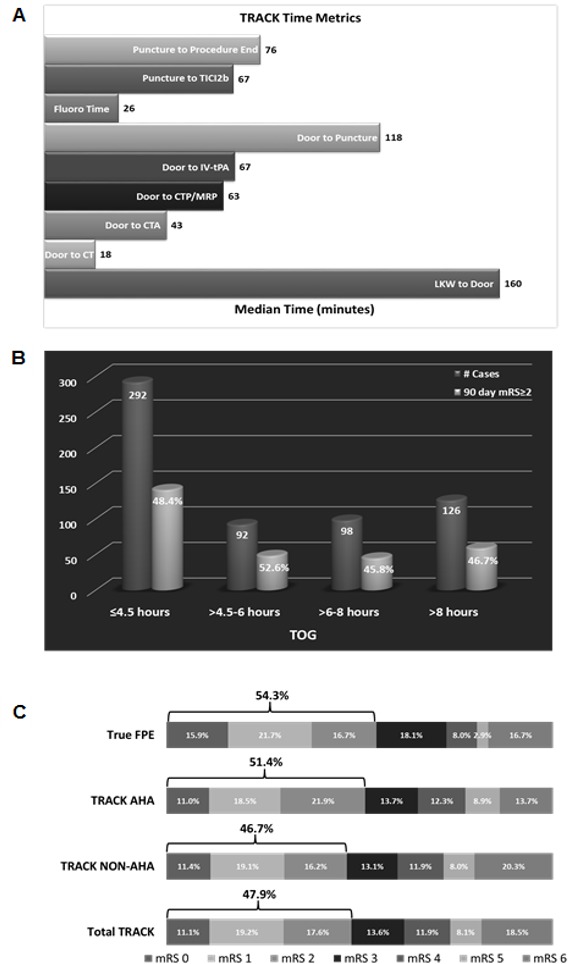
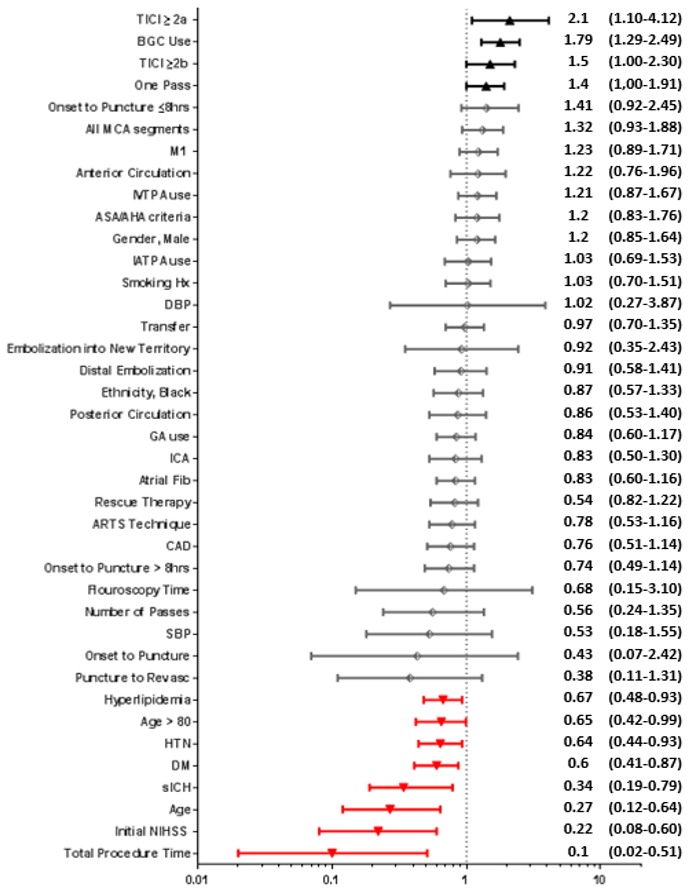
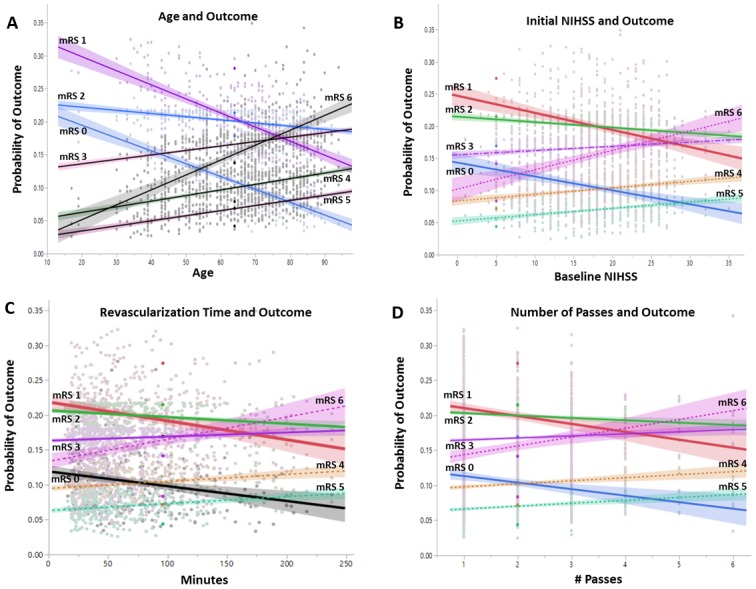
Results: A total of 634patients were included. Mean age was 66.1±14.8 years and mean baseline NIH Stroke Scale (NIHSS) score was 17.4±6.7; 86.7% had an anterior circulation occlusion. Mean time from symptom onset to puncture and time to revascularization were 363.1±264.5 min and 78.8±49.6 min, respectively. 80.3% achieved TICI ≥2b. 90-day mRS ≤2 was achieved in 47.9%, compared with 51.4% when restricting the analysis to the anterior circulation and within 6 hours (similar to recent AHA/ASA guidelines), and 54.3% for those who achieved complete revascularization. The 90-day mortality rate was 19.8%. Independent predictors of clinical outcome included age, baseline NIHSS, use of balloon guide catheter, revascularization, and sICH.
Conclusion: The TRACK Registry results demonstrate the generalizability of the recent thrombectomy RCTs in real-world clinical practice. No differences in clinical and angiographic outcomes were shown between patients treated within the AHA/ASA guidelines and those treated outside the recommendations.
Keywords: mechanical; revascularization; stent-retriever; stroke; thrombectomy; trevo.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: IL is consultant for Metronic, Stryker, Penumbra, and Cordis. MM is consultant for Claret Medical, Nogueira-Stryker Neurovascular (Trevo-2 Trial Principal Investigator – modest; DAWN Trial Principal Investigator – no compensation, TREVO Registry Steering Committee – no compensation), Medtronic (SWIFT Trial Steering Committee – modest; SWIFT-Prime Trial Steering Committee – no compensation; STAR Trial Angiographic Core Lab – significant), Penumbra (3D Separator Trial Executive Committee – no compensation), Neuravi (ARISE-2 Steering Committee – no compensation), Genentech (Physician Advisory Board – modest), Allm Inc (Physician Advisory Board – no compensation), Editor-In-Chief Interventional Neurology Journal (no compensation). SRS is a consultant for Stryker Neurovascular. OOZ is overall PI for TRACK – no compensation, Arise II – modest, Co-PI Therapy Trial – modest, Steering committee STRATIS registry – modest.
Figures
References
-
- English JD, Yavagal DR, Gupta R, et al. Mechanical thrombectomy-ready comprehensive stroke center requirements and endovascular stroke systems of care: recommendations from the Endovascular Stroke Standards Committee of the Society of Vascular and Interventional Neurology (SVIN). Interv Neurol 2016;4:138–50. 10.1159/000442715 - DOI - PMC - PubMed
-
- Powers WJ, Derdeyn CP, Biller J, et al. American Heart Association/American Stroke Association focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2015;2015:3020–35. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical